The Bobby R. Alford Department of Otolaryngology - Head and Neck Surgery, Baylor College of Medicine and The Hearing Center at Texas Children's Hospital, Houston, Texas, USA.
Otol Neurotol. 2011 Feb;32(2):259-64. doi: 10.1097/MAO.0b013e31820160fa.
Selection of diagnostic tests for children with sensorineural hearing loss (SNHL) is influenced by clinical suspicion. Testing results reported in the literature are similarly biased. We evaluate the usefulness of a comprehensive diagnostic battery for each child.
Retrospective review.
Tertiary care university hospital.
A total of 270 children referred for severe to profound SNHL between January 2002 and June 2009.
Results of the following were reviewed: magnetic resonance imaging, computed tomography, renal ultrasound, electrocardiography, fluorescent treponemal antibody absorption test, connexin 26 sequencing, genetic consultation, and ophthalmologic consultation.
Diagnostic yield of each test was determined.
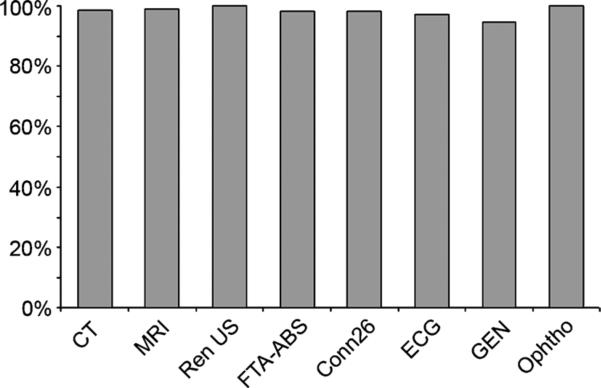
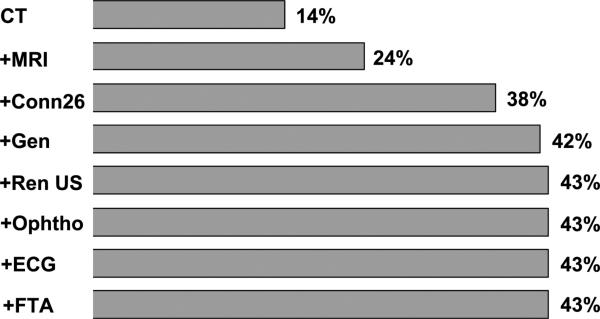
Each diagnostic test or consultation was completed by at least 95% of patients for whom it was ordered. Magnetic resonance imaging revealed abnormalities explaining SNHL in 24% of patients. Computed tomography showed inner ear anomalies in 18% of patients. Biallelic connexin 26 mutations were found in 15%. Renal ultrasound found anomalies in 4% of patients. Electrocardiography found 1% of patients with prolonged QT intervals. Fluorescent treponemal antibody absorption test result was positive in 0.5%. Genetic consultation found a genetic cause for hearing loss in 25%. Ophthalmologic consultation found abnormalities associated with hearing loss in 8%.
Diagnostic radiologic imaging is the highest yielding test for evaluating children with SNHL. Connexin 26 sequencing identifies a nearly nonoverlapping subset of children compared with imaging. Specialty consultations, particularly from a clinical geneticist, can improve diagnostic yield. Other tests, although of lower diagnostic yield for SNHL, can identify important diseases that significantly affect patient health.
儿童感音神经性听力损失(SNHL)的诊断测试选择受到临床怀疑的影响。文献中报告的测试结果也存在类似的偏差。我们评估了为每个孩子提供全面诊断电池的有用性。
回顾性审查。
三级保健大学医院。
2002 年 1 月至 2009 年 6 月期间,共 270 名因严重至重度 SNHL 而转介的儿童。
审查了以下结果:磁共振成像、计算机断层扫描、肾脏超声、心电图、荧光密螺旋体抗体吸收试验、连接蛋白 26 测序、遗传咨询和眼科咨询。
确定每项测试的诊断产量。
为其订购的患者中,至少有 95%完成了每项诊断测试或咨询。磁共振成像显示 24%的患者存在解释 SNHL 的异常。计算机断层扫描显示 18%的患者存在内耳异常。双等位基因连接蛋白 26 突变在 15%的患者中发现。肾脏超声在 4%的患者中发现异常。心电图发现 1%的患者 QT 间期延长。荧光密螺旋体抗体吸收试验结果阳性为 0.5%。遗传咨询发现听力损失的遗传原因在 25%的患者中。眼科咨询发现与听力损失相关的异常在 8%的患者中。
诊断性放射影像学是评估 SNHL 儿童的最高产测试。与成像相比,连接蛋白 26 测序确定了一个几乎没有重叠的子集的儿童。特别是来自临床遗传学家的专业咨询可以提高诊断产量。其他测试,尽管对 SNHL 的诊断产量较低,但可以识别对患者健康有重大影响的重要疾病。