Department of Radiation Oncology, Hospital Israelita Albert Einstein, Av, Albert Einstein, 627, São Paulo-SP-05651-901-Brazil.
Radiat Oncol. 2010 Dec 14;5:117. doi: 10.1186/1748-717X-5-117.
This retrospective analysis reports on the comparative outcome of acute gastrointestinal (GI) and genitourinary (GU) toxicities between conformal radiation therapy (CRT) and intensity modulated radiation therapy (IMRT) techniques in the treatment of patients with pelvic tumors.
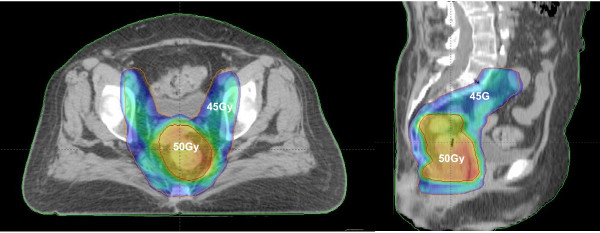
From January 2002 to December 2008, 69 patients with pelvic tumors underwent whole pelvic CRT and 65 underwent whole pelvic IMRT to treat pelvic lymph nodes and primary tumor regions. Total dose to the whole pelvis ranged from 50 to 50.4 Gy in 25 to 28 daily fractions. Chemotherapy (CT) regimen, when employed, was based upon primary tumor. Acute GI and GU toxicities were graded by RTOG/EORTC acute radiation morbidity criteria.
Absence of GI symptoms during radiotherapy (grade 0) was more frequently observed in the IMRT group (43.1% versus 8.7; p < 0.001) and medication for diarrhea (Grade 2) was more frequently used in the CRT group (65.2% versus 38.5%; p = 0.002). Acute GI grade 1 and 3 side effects incidence was similar in both groups (18.5% versus 18.8%; p = 0.95 and 0% versus 7.2%; p = 0.058, respectively). Incidence of GU toxicity was similar in both groups (grade 0: 61.5% versus 66.6%, p = 0.54; grade 1: 20% versus 8.7%, p = 0.06; grade 2: 18.5% versus 23.5%, p = 0.50 and grade 3: 0% versus 1.5%, p > 0.99).
This comparative case series shows less grade 2 acute GI toxicity in patients treated with whole pelvic IMRT in comparison with those treated with CRT. Incidence of acute GU toxicity was similar in both groups.
本回顾性分析报告比较了盆腔肿瘤患者接受适形放疗(CRT)和调强放疗(IMRT)技术治疗时急性胃肠道(GI)和泌尿生殖系统(GU)毒性的结果。
2002 年 1 月至 2008 年 12 月,69 例盆腔肿瘤患者接受全盆腔 CRT,65 例接受全盆腔 IMRT,以治疗盆腔淋巴结和原发肿瘤区域。全盆腔总剂量为 50 至 50.4Gy,分 25 至 28 次每日分割。化疗(CT)方案根据原发肿瘤而定。急性 GI 和 GU 毒性采用 RTOG/EORTC 急性放射损伤标准分级。
IMRT 组中(43.1%比 8.7%;p < 0.001)放疗期间胃肠道症状(0 级)的发生率更高,而 CRT 组中腹泻药物治疗(2 级)的使用率更高(65.2%比 38.5%;p = 0.002)。两组急性 GI 1 级和 3 级副作用发生率相似(18.5%比 18.8%;p = 0.95 和 0%比 7.2%;p = 0.058)。两组 GU 毒性发生率相似(0 级:61.5%比 66.6%,p = 0.54;1 级:20%比 8.7%,p = 0.06;2 级:18.5%比 23.5%,p = 0.50;3 级:0%比 1.5%,p > 0.99)。
本病例系列比较研究表明,接受全盆腔 IMRT 治疗的患者急性 2 级 GI 毒性低于接受 CRT 治疗的患者。两组急性 GU 毒性发生率相似。