Menkarios Cathy, Azria David, Laliberté Benoit, Moscardo Carmen Llacer, Gourgou Sophie, Lemanski Claire, Dubois Jean-Bernard, Aillères Norbert, Fenoglietto Pascal
Département de Radio-Oncologie, Hôpital Maisonneuve-Rosemont, Montréal, Canada.
Radiat Oncol. 2007 Nov 15;2:41. doi: 10.1186/1748-717X-2-41.
To compare the dosimetric advantage of three different intensity-modulated radiation therapy (IMRT) plans to a three dimensional (3D) conventional radiation treatment for anal cancer with regards to organs-at-risk (OAR) avoidance, including iliac bone marrow.
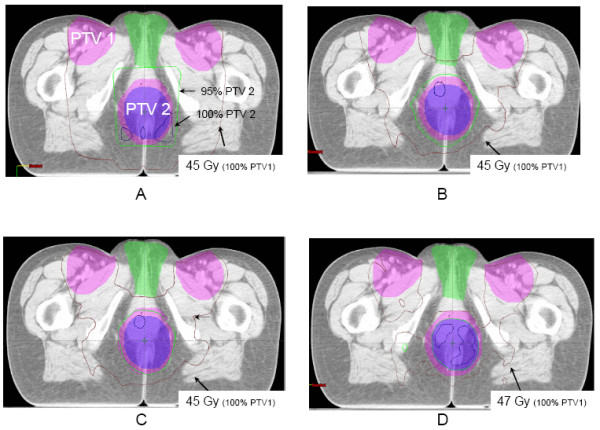
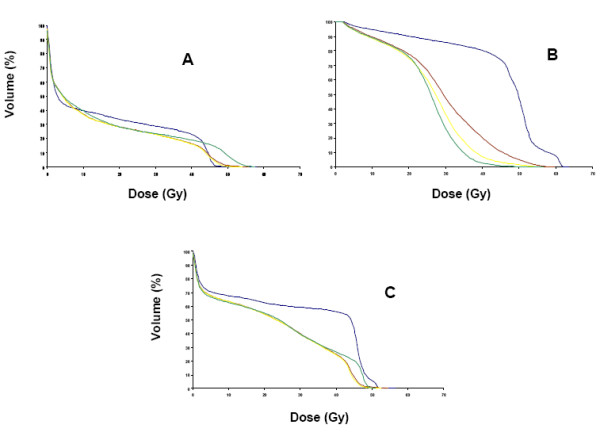
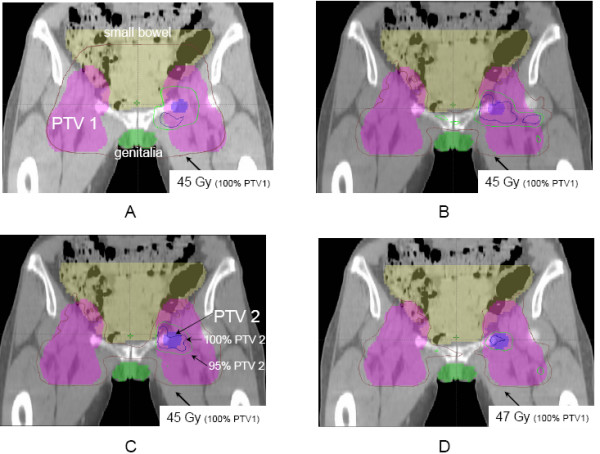
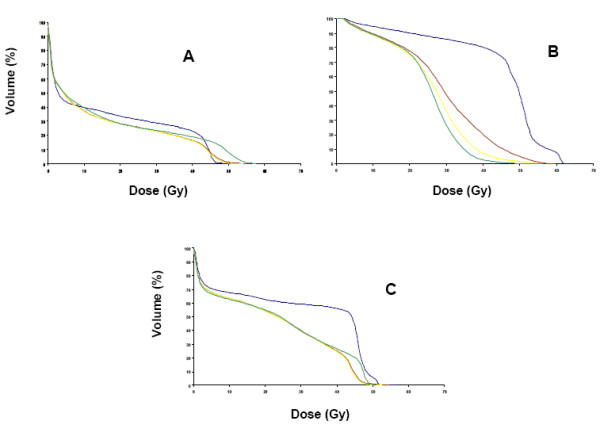
Five patients with T1-3 N0-1 anal cancer and five with T4 and/or N2-3 tumors were selected. Clinical tumor volume (CTV) included tumor, anal canal and inguinal, peri-rectal, and internal/external iliac nodes (plus pre-sacral nodes for T4/N2-3 tumors). Four plans were generated: (A) AP/PA with 3D conformal boost, (B) pelvic IMRT with conformal boost (C) pelvic IMRT with IMRT boost and (D) IMRT with simultaneous integrated boost (SIB). The dose for plans (A) to (C) was 45 Gy/25 followed by a 14.4 Gy/8 boost, and the total dose for plan (D) (SIB) was 59.4 Gy/33. Coverage of both PTV and the volume of OAR (small bowel, genitalia, iliac crest and femoral heads) receiving more than 10, 20, 30, and 40 Gy (V10, V20, V30, V40) were compared using non parametric statistics.
Compared to plan (A), IMRT plans (B) to (D) significantly reduced the V30 and V40 of small bowel, bladder and genitalia for all patients. The V10 and V20 of iliac crests were similar for the N0-1 group but were significantly reduced with IMRT for the N2-3/T4 group (V20 for A = 50.2% compared to B = 33%, C = 32.8%, D = 34.3%). There was no statistical difference between 2-phase (arm C) and single-phase (SIB, arm D) IMRT plans.
IMRT is superior to 3D conformal radiation treatment for anal carcinoma with respect to OAR sparing, including bone marrow sparing.
比较三种不同的调强放射治疗(IMRT)计划与三维(3D)常规放射治疗在肛管癌中对危及器官(OAR)的避让优势,包括髂骨髓。
选取5例T1-3 N0-1期肛管癌患者和5例T4和/或N2-3期肿瘤患者。临床靶体积(CTV)包括肿瘤、肛管以及腹股沟、直肠周围和髂内/外淋巴结(T4/N2-3期肿瘤还包括骶前淋巴结)。生成了四个计划:(A)前后野(AP/PA)联合3D适形加量,(B)盆腔IMRT联合适形加量,(C)盆腔IMRT联合IMRT加量,以及(D)IMRT同步整合加量(SIB)。计划(A)至(C)的剂量为45 Gy/25次,随后14.4 Gy/8次加量,计划(D)(SIB)的总剂量为59.4 Gy/33次。使用非参数统计比较了计划靶体积(PTV)的覆盖情况以及接受超过10、20、30和40 Gy(V10、V20、V30、V40)的OAR(小肠、生殖器、髂嵴和股骨头)体积。
与计划(A)相比,IMRT计划(B)至(D)显著降低了所有患者小肠、膀胱和生殖器的V30和V40。N0-1组髂嵴的V10和V20相似,但N2-3/T4组IMRT使其显著降低(A组的V20为50.2%,相比之下B组为33%,C组为32.8%,D组为34.3%)。两阶段(C组)和单阶段(SIB,D组)IMRT计划之间无统计学差异。
在包括骨髓保护在内的OAR保护方面,IMRT优于肛管癌三维适形放射治疗。