Department of Human Oncology, University of Wisconsin Carbone Cancer Center, School of Medicine and Public Health, Madison, WI 53792, USA.
Int J Radiat Oncol Biol Phys. 2012 Jan 1;82(1):184-90. doi: 10.1016/j.ijrobp.2010.09.018. Epub 2010 Dec 14.
Toxicity concerns have limited pelvic nodal prescriptions to doses that may be suboptimal for controlling microscopic disease. In a prospective trial, we tested whether image-guided intensity-modulated radiation therapy (IMRT) can safely deliver escalated nodal doses while treating the prostate with hypofractionated radiotherapy in 5½ weeks.
Pelvic nodal and prostatic image-guided IMRT was delivered to 53 National Comprehensive Cancer Network (NCCN) high-risk patients to a nodal dose of 56 Gy in 2-Gy fractions with concomitant treatment of the prostate to 70 Gy in 28 fractions of 2.5 Gy, and 50 of 53 patients received androgen deprivation for a median duration of 12 months.
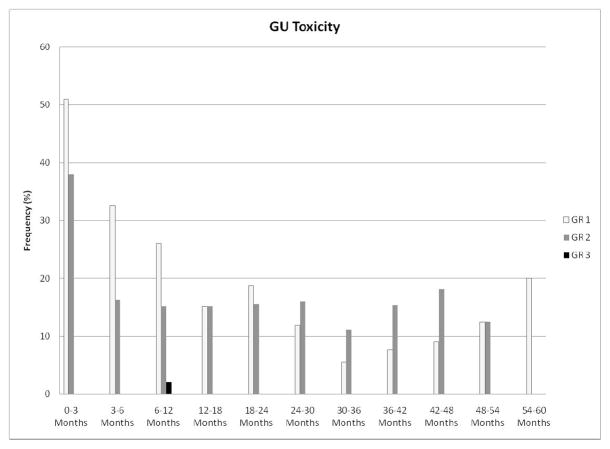
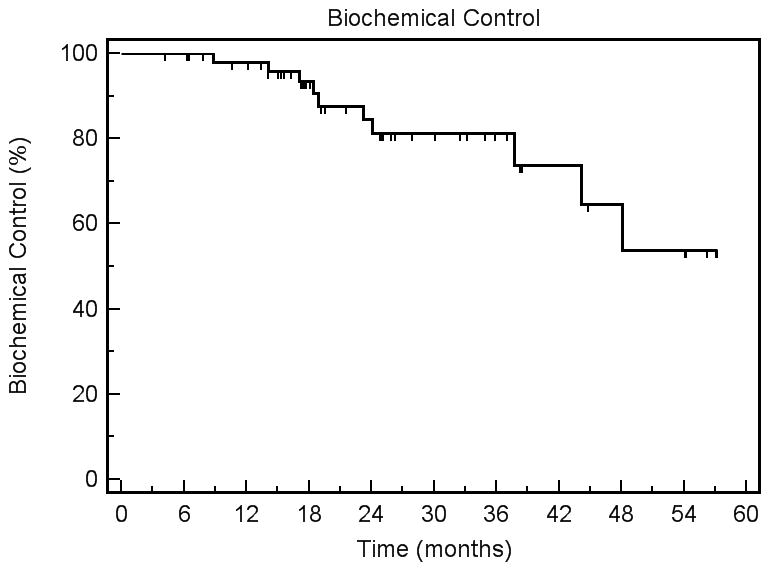
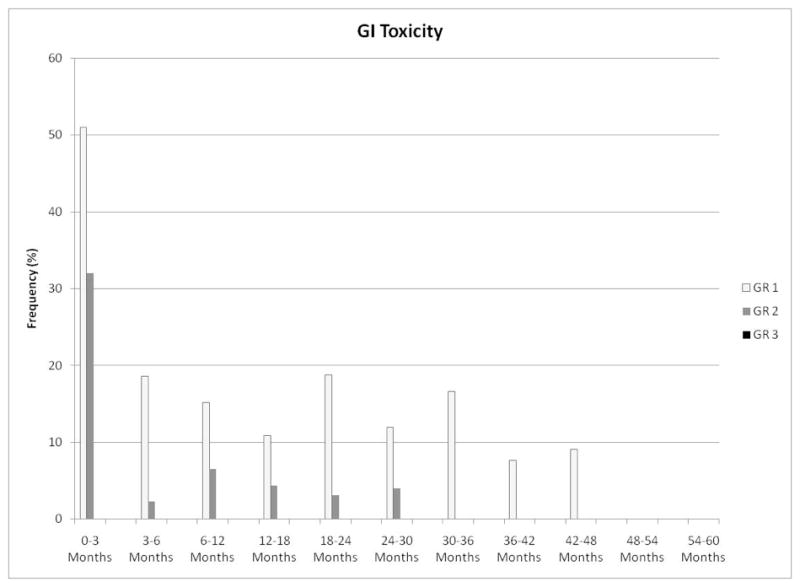
The median follow-up time was 25.4 months (range, 4.2-57.2). No early Grade 3 Radiation Therapy Oncology Group or Common Terminology Criteria for Adverse Events v.3.0 genitourinary (GU) or gastrointestinal (GI) toxicities were seen. The cumulative actuarial incidence of Grade 2 early GU toxicity (primarily alpha blocker initiation) was 38%. The rate was 32% for Grade 2 early GI toxicity. None of the dose-volume descriptors correlated with GU toxicity, and only the volume of bowel receiving ≥30 Gy correlated with early GI toxicity (p = 0.029). Maximum late Grades 1, 2, and 3 GU toxicities were seen in 30%, 25%, and 2% of patients, respectively. Maximum late Grades 1 and 2 GI toxicities were seen in 30% and 8% (rectal bleeding requiring cautery) of patients, respectively. The estimated 3-year biochemical control (nadir + 2) was 81.2 ± 6.6%. No patient manifested pelvic nodal failure, whereas 2 experienced paraaortic nodal failure outside the field. The six other clinical failures were distant only.
Pelvic IMRT nodal dose escalation to 56 Gy was delivered concurrently with 70 Gy of hypofractionated prostate radiotherapy in a convenient, resource-efficient, and well-tolerated 28-fraction schedule. Pelvic nodal dose escalation may be an option in any future exploration of potential benefits of pelvic radiation therapy in high-risk prostate cancer patients.
毒性问题限制了盆腔淋巴结的剂量,使其可能无法充分控制微观疾病。在一项前瞻性试验中,我们测试了图像引导的强度调制放射治疗(IMRT)是否可以在 5 周半的时间内安全地给予递增的淋巴结剂量,同时对前列腺进行低分割放射治疗。
对 53 例 NCCN 高危患者进行盆腔淋巴结和前列腺图像引导的 IMRT,给予 56 Gy 的淋巴结剂量,2 Gy/次,同时给予前列腺 70 Gy 的剂量,28 次/次,2.5 Gy,53 例中有 50 例患者接受中位持续时间为 12 个月的雄激素剥夺治疗。
中位随访时间为 25.4 个月(范围 4.2-57.2)。未观察到早期 3 级放射治疗肿瘤学组或常见不良事件术语标准 3.0 版泌尿生殖系统(GU)或胃肠道(GI)毒性。累积发生率为 38%的 2 级早期 GU 毒性(主要是α阻滞剂的开始)。2 级早期 GI 毒性的发生率为 32%。没有任何剂量-体积描述符与 GU 毒性相关,只有接受≥30 Gy 的肠道体积与早期 GI 毒性相关(p = 0.029)。30%、25%和 2%的患者分别出现最大晚期 1、2 和 3 级 GU 毒性。30%和 8%(需要电灼的直肠出血)的患者出现最大晚期 1 级和 2 级 GI 毒性。估计 3 年生化控制(最低点+2)为 81.2±6.6%。没有患者出现盆腔淋巴结失败,而 2 例患者在野外发生了paraaortic 淋巴结失败。其他 6 例临床失败均为远处转移。
在方便、资源高效和耐受性良好的 28 次分割方案中,将盆腔 IMRT 淋巴结剂量递增至 56 Gy,同时给予 70 Gy 的低分割前列腺放射治疗。在高危前列腺癌患者中,盆腔放疗的潜在获益的任何未来探索中,增加盆腔淋巴结剂量可能是一种选择。