London School of Hygiene and Tropical Medicine, London, UK.
Lancet. 2011 Jan 1;377(9759):52-62. doi: 10.1016/S0140-6736(10)61457-2. Epub 2010 Dec 20.
Helminth infections affect the human immune response. We investigated whether prenatal exposure to and treatment of maternal helminth infections affects development of an infant's immune response to immunisations and unrelated infections.
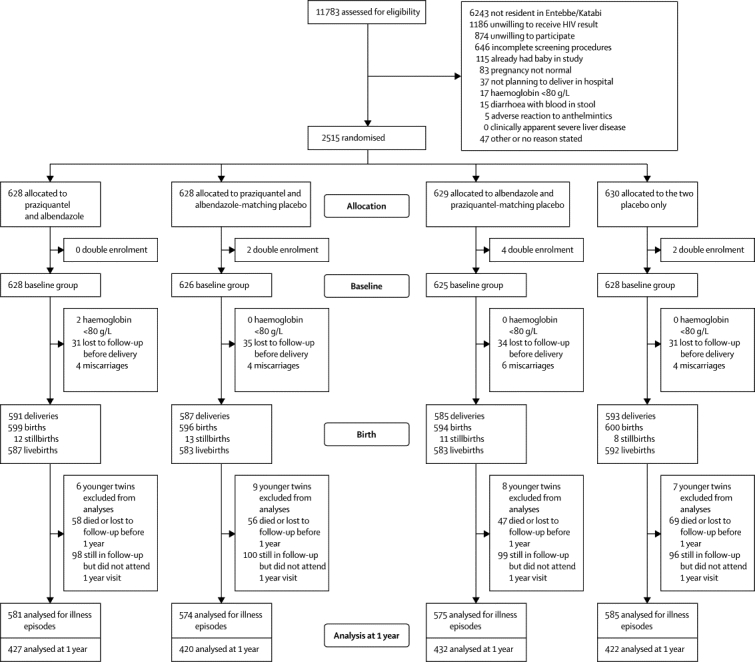
In this randomised, double-blind, placebo-controlled trial, we enrolled 2507 women in the second or third trimester of pregnancy who were planning to deliver in Entebbe General Hospital, Entebbe, Uganda. With a computer-generated random number sequence in blocks of 100, we assigned patients to 440 mg albendazole and 40 mg/kg praziquantel (n=628), 440 mg albendazole and a praziquantel-matching placebo (n=625), 40 mg/kg praziquantel and an albendazole-matching placebo (n=626), or an albendazole-matching placebo and praziquantel-matching placebo (n=628). All participants and hospital staff were masked to allocation. Primary outcomes were immune response at age 1 year to BCG, tetanus, and measles immunisation; incidence of infectious diseases during infancy; and vertical HIV transmission. Analysis was by intention-to-treat. This trial is registered, number ISRCTN32849447.
Data were available at delivery for 2356 women, with 2345 livebirths; 2115 (90%) of liveborn infants remained in follow-up at 1 year of age. Neither albendazole nor praziquantel treatments affected infant response to BCG, tetanus, or measles immunisation. However, in infants of mothers with hookworm infection, albendazole treatment reduced interleukin-5 (geometric mean ratio 0·50, 95% CI 0·30-0·81, interaction p=0·02) and interleukin-13 (0·52, 0·34-0·82, 0·0005) response to tetanus toxoid. The rate per 100 person-years of malaria was 40·9 (95% CI 38·3-43·7), of diarrhoea was 134·1 (129·2-139·2), and of pneumonia was 22·3 (20·4-24·4). We noted no effect on infectious disease incidence for albendazole treatment (malaria [hazard ratio 0·95, 95% CI 0·79-1.14], diarrhoea [1·06, 0·96-1·16], pneumonia [1·11, 0·90-1·38]) or praziquantel treatment (malaria [1·00, 0·84-1·20], diarrhoea [1·07, 0·98-1·18], pneumonia [1·00, 0·80-1·24]). In HIV-exposed infants, 39 (18%) were infected at 6 weeks; vertical transmission was not associated with albendazole (odds ratio 0·70, 95% CI 0·35-1·42) or praziquantel (0·60, 0·29-1·23) treatment.
These results do not accord with the recently advocated policy of routine antenatal anthelmintic treatment, and the value of such a policy may need to be reviewed.
Wellcome Trust.
寄生虫感染会影响人体的免疫反应。我们研究了母体寄生虫感染的产前暴露和治疗是否会影响婴儿对免疫接种和无关感染的免疫反应的发展。
在这项随机、双盲、安慰剂对照试验中,我们招募了 2507 名计划在乌干达恩德培总医院分娩的妊娠第二或第三期的孕妇。根据计算机生成的随机数序列,我们将患者分为 4 组:440mg 阿苯达唑和 40mg/kg 吡喹酮(n=628)、440mg 阿苯达唑和吡喹酮安慰剂(n=625)、40mg/kg 吡喹酮和阿苯达唑安慰剂(n=626)或阿苯达唑安慰剂和吡喹酮安慰剂(n=628)。所有参与者和医院工作人员对分组均不知情。主要结局是婴儿在 1 岁时对卡介苗、破伤风和麻疹免疫接种的免疫反应;婴儿期感染性疾病的发生率;以及垂直传播的艾滋病毒感染。分析采用意向治疗。这项试验已在 ISRCTN 注册,编号为 ISRCTN32849447。
在分娩时,2356 名女性中有数据可用,2345 名活产;2115 名(90%)的活产婴儿在 1 岁时仍在随访中。阿苯达唑和吡喹酮治疗均不影响婴儿对卡介苗、破伤风或麻疹免疫接种的反应。然而,在感染钩虫的母亲的婴儿中,阿苯达唑治疗降低了对破伤风类毒素的白细胞介素-5(几何平均比 0.50,95%CI 0.30-0.81,交互作用 p=0.02)和白细胞介素-13(0.52,0.34-0.82,p=0.0005)反应。每 100 人年疟疾发生率为 40.9(95%CI 38.3-43.7),腹泻发生率为 134.1(129.2-139.2),肺炎发生率为 22.3(20.4-24.4)。我们没有发现阿苯达唑治疗(疟疾[风险比 0.95,95%CI 0.79-1.14]、腹泻[1.06,0.96-1.16]、肺炎[1.11,0.90-1.38])或吡喹酮治疗(疟疾[1.00,0.84-1.20]、腹泻[1.07,0.98-1.18]、肺炎[1.00,0.80-1.24])对感染性疾病发生率有影响。在暴露于艾滋病毒的婴儿中,有 39 名(18%)在 6 周时感染;垂直传播与阿苯达唑(比值比 0.70,95%CI 0.35-1.42)或吡喹酮(0.60,0.29-1.23)治疗无关。
这些结果与最近提倡的常规产前驱虫治疗政策不一致,因此可能需要重新评估这种政策的价值。
惠康信托基金会。