New Zealand Familial GI Cancer Registry, Auckland City Hospital, New Zealand.
Gut. 2011 Jul;60(7):950-7. doi: 10.1136/gut.2010.228056. Epub 2010 Dec 30.
Surgical management of colon cancer for patients with Lynch syndrome who carry a mismatch repair (MMR) gene mutation is controversial. The decision to remove more or less of the colon involves the consideration of a relatively high risk of metachronous colorectal cancer (CRC) with the impact of more extensive surgery.
To estimate and compare the risks of metachronous CRC for patients with Lynch syndrome undergoing either segmental or extensive (subtotal or total) resection for first colon cancer.
Risk of metachronous CRC was estimated for 382 MMR gene mutation carriers (172 MLH1, 167 MSH2, 23 MSH6 and 20 PMS2) from the Colon Cancer Family Registry, who had surgery for their first colon cancer, using retrospective cohort analysis. Age-dependent cumulative risks of metachronous CRC were calculated using the Kaplan-Meier method. Risk factors for metachronous CRC were assessed by a Cox proportional hazards regression.
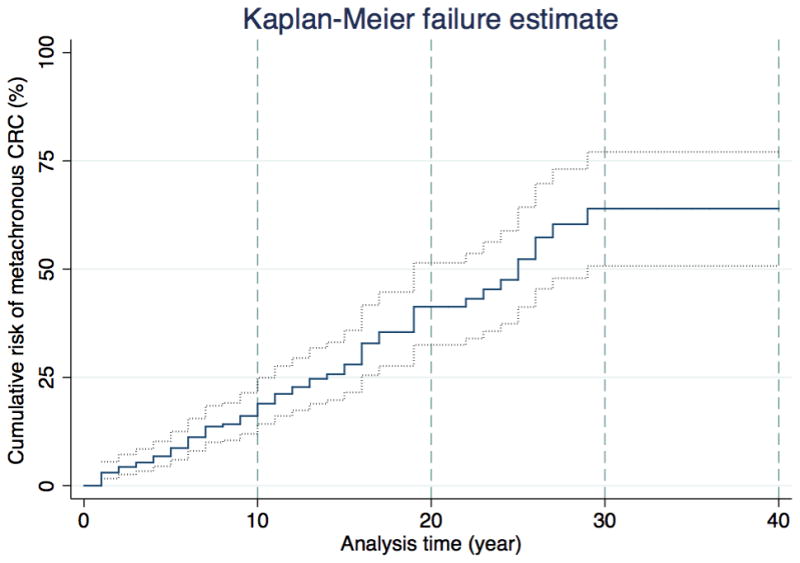
None of 50 subjects who had extensive colectomy was diagnosed with metachronous CRC (incidence rate 0.0; 95% CI 0.0 to 7.2 per 1000 person-years). Of 332 subjects who had segmental resections, 74 (22%) were diagnosed with metachronous CRC (incidence rate 23.6; 95% CI 18.8 to 29.7 per 1000 person-years). For those who had segmental resections, incidence was statistically higher than for those who had extensive surgery (P <0.001). Cumulative risk of metachronous CRC was 16% (95% CI 10% to 25%) at 10 years, 41% (95% CI 30% to 52%) at 20 years and 62% (95% CI 50% to 77%) at 30 years after segmental colectomy. Risk of metachronous CRC reduced by 31% (95% CI 12% to 46%; p=0.002) for every 10 cm of bowel removed.
Patients with Lynch syndrome with first colon cancer treated with more extensive colonic resection have a lower risk of metachronous CRC than those receiving less extensive surgery. This finding will better inform decision-making about the extent of primary surgical resection.
对于携带错配修复(MMR)基因突变的林奇综合征患者的结肠癌手术治疗存在争议。决定切除更多或更少的结肠涉及到考虑相对较高的结直肠肿瘤(CRC)风险,这与更广泛的手术有关。
评估并比较林奇综合征患者首次结肠癌行节段或广泛(次全或全)切除术的 CRC 异时性风险。
使用回顾性队列分析,从结肠癌家族登记处(Colon Cancer Family Registry)中对 382 名 MMR 基因突变携带者(172 名 MLH1、167 名 MSH2、23 名 MSH6 和 20 名 PMS2)进行了 CRC 异时性风险的估计,这些患者接受了首次结肠癌手术。使用 Kaplan-Meier 方法计算年龄相关的 CRC 异时性累积风险。使用 Cox 比例风险回归评估 CRC 异时性的危险因素。
50 名接受广泛结肠切除术的患者中无一例被诊断为 CRC(发病率为 0.0;95%CI 0.0 至 7.2/1000 人年)。在 332 名接受节段切除术的患者中,74 名(22%)被诊断为 CRC(发病率为 23.6;95%CI 18.8 至 29.7/1000 人年)。对于接受节段切除术的患者,发病率明显高于接受广泛手术的患者(P <0.001)。节段性结肠切除术后 10 年 CRC 异时性的累积风险为 16%(95%CI 10%至 25%),20 年为 41%(95%CI 30%至 52%),30 年为 62%(95%CI 50%至 77%)。每切除 10cm 肠管,CRC 异时性的风险降低 31%(95%CI 12%至 46%;p=0.002)。
对于首次患有结肠癌的林奇综合征患者,行更广泛的结肠切除术治疗的 CRC 异时性风险低于接受不广泛手术的患者。这一发现将更好地为主要手术切除范围的决策提供依据。