UCSF Benioff Children's Hospital, Department of Surgery, University of California, San Francisco, CA 94143, USA.
J Thorac Cardiovasc Surg. 2011 Feb;141(2):400-6. doi: 10.1016/j.jtcvs.2010.10.047.
Bidirectional cavopulmonary anastomosis has been performed without cardiopulmonary bypass for some single-ventricle heart defects. Limited data are available for the outcomes of off-pump bidirectional cavopulmonary anastomosis in infants with hypoplastic left heart syndrome. The purpose of this study is to determine the early outcomes for stage II palliation of hypoplastic left heart syndrome without cardiopulmonary bypass.
This is a retrospective review of infants having surgical palliation of hypoplastic left heart syndrome from April 2003 to March 2010 at a single institution.
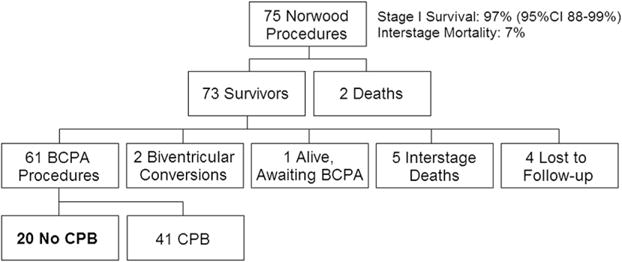
Seventy-five infants had a modified Norwood procedure, 65 with a right ventricle-pulmonary artery conduit, 10 with an aortopulmonary shunt, 2 with atrioventricular valve repair, and 3 with extracorporeal life support. Sixty-eight patients had hypoplastic left heart syndrome or one of its variants, and 7 had other single-ventricle lesions. There were 2 stage I deaths. Stage I survival was 97% (95% confidence interval, 88%-99%). Another 5 infants succumbed in the interstage period. Of the 68 stage I and interstage survivors, 61 had bidirectional cavopulmonary anastomoses, 20 without cardiopulmonary bypass. Median age was 6 months (range, 4-13 months), and median weight was 6.1 kg (range, 5.2-9.0 kg). There were no conversions to cardiopulmonary bypass when off-pump bidirectional cavopulmonary anastomosis was attempted. There were no hospital deaths. Median ventilation duration was 10 hours (range, 6-18 hours), and length of stay was 5 days (range, 4-9 days). Follow-up was available on all infants at a median duration of 17 months (range, 3-43 months), with no unplanned reinterventions.
Bidirectional cavopulmonary anastomosis without the use of cardiopulmonary bypass can be performed safely and with low mortality for selected infants with hypoplastic left heart syndrome. Midterm to long-term outcomes remain to be determined.
对于某些单心室心脏缺陷,已经可以在不使用体外循环的情况下进行双向腔肺吻合术。对于左心发育不全综合征患儿,体外循环下双向腔肺吻合术的结果数据有限。本研究旨在确定无体外循环的左心发育不全综合征二期姑息手术的早期结果。
这是对 2003 年 4 月至 2010 年 3 月期间在一家机构接受左心发育不全综合征姑息手术的婴儿进行的回顾性研究。
75 例婴儿行改良的 Norwood 手术,其中 65 例采用右心室-肺动脉导管,10 例采用主动脉-肺动脉分流术,2 例行房室瓣修复术,3 例行体外生命支持。68 例患儿患有左心发育不全综合征或其变异型,7 例患儿患有其他单心室病变。有 2 例一期死亡。一期存活率为 97%(95%置信区间,88%-99%)。另有 5 例患儿在中间期死亡。在 68 例一期和中间期存活者中,61 例行双向腔肺吻合术,其中 20 例未行体外循环。中位年龄为 6 个月(范围,4-13 个月),中位体重为 6.1kg(范围,5.2-9.0kg)。当尝试进行非体外循环下双向腔肺吻合术时,无转换为体外循环。无院内死亡。中位通气时间为 10 小时(范围,6-18 小时),住院时间为 5 天(范围,4-9 天)。所有婴儿的随访时间中位数为 17 个月(范围,3-43 个月),无计划再干预。
对于选定的左心发育不全综合征患儿,在不使用体外循环的情况下,可以安全地进行双向腔肺吻合术,且死亡率低。中期至长期结果仍有待确定。