Department of Breast Medical Oncology, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Boulevard, Unit 1354, Houston, Texas 77030, USA.
Oncologist. 2011;16(2):155-64. doi: 10.1634/theoncologist.2010-0350. Epub 2011 Jan 25.
Limited information is available about the optimal management and clinical outcome of bone-only metastases in breast cancer patients. The objective of this study was to define prognostic factors for patients with bone-only metastases. Our second objective was to compare progression-free survival (PFS) and overall survival (OS) between patients with hormone receptor (HR)(+) tumors and bone-only metastases who received combinatory therapy (chemotherapy followed by endocrine therapy, or endocrine therapy combined with molecular targeted therapy) and those treated with endocrine or chemotherapy alone.
We retrospectively identified 351 breast cancer patients diagnosed with bone-only metastasis in 1997-2008 at our institution.
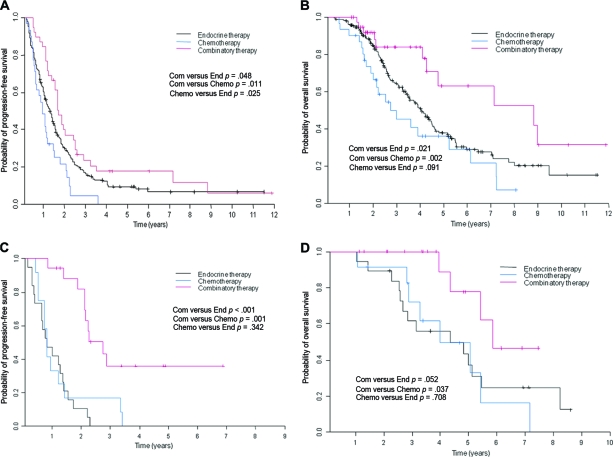
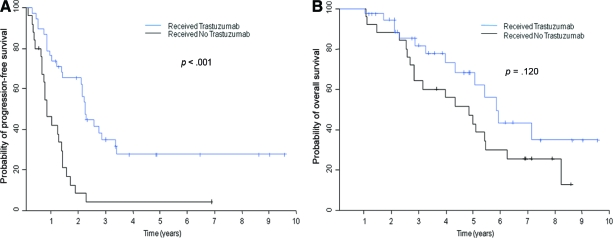
Patients with metastasis detected at the time of their primary breast cancer diagnosis (rather than at recurrence), a single metastasis, or asymptomatic bone disease had a longer PFS interval, and patients with a performance status of 0-1, a single metastasis, or asymptomatic bone disease had a longer OS time. Among patients with HR(+) human epidermal growth factor receptor (HER)-2(-) disease, combinatory therapy was associated with longer PFS and OS times than with endocrine therapy. In multivariate analyses, combinatory therapy was not associated with longer PFS or OS times than with endocrine therapy. Among patients with HER-2(+) disease, trastuzumab led to a longer PFS interval but no difference in the OS time.
Our results indicate that, for HR(+) disease, a prospective trial of chemotherapy followed by endocrine therapy is warranted to determine whether it prolongs survival more than endocrine therapy alone in patients with bone-only metastases.
关于乳腺癌患者仅有骨转移的最佳治疗和临床转归,相关信息有限。本研究旨在明确仅有骨转移的乳腺癌患者的预后因素。我们的次要目标是比较接受联合治疗(化疗后继以内分泌治疗,或内分泌治疗联合分子靶向治疗)与仅接受内分泌或化疗治疗的激素受体(HR)阳性肿瘤且仅有骨转移患者的无进展生存期(PFS)和总生存期(OS)。
我们回顾性分析了 1997-2008 年在我院诊断为仅有骨转移的 351 例乳腺癌患者。
在初诊时(而非复发时)、单一转移灶或无症状骨疾病的患者 PFS 间隔较长,体力状态为 0-1、单一转移灶或无症状骨疾病的患者 OS 时间较长。在 HR 阳性人表皮生长因子受体(HER)-2 阴性疾病患者中,联合治疗与更长的 PFS 和 OS 时间相关,优于内分泌治疗。多变量分析显示,联合治疗与内分泌治疗相比,并不延长 PFS 或 OS 时间。在 HER-2 阳性疾病患者中,曲妥珠单抗可延长 PFS 间隔,但对 OS 时间无影响。
我们的结果表明,对于 HR 阳性疾病,需要开展前瞻性化疗后继以内分泌治疗试验,以确定在仅有骨转移的患者中,与单独内分泌治疗相比,该方案是否可延长生存。