Division of Cardiology, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea.
Korean Circ J. 2010 Dec;40(12):639-44. doi: 10.4070/kcj.2010.40.12.639. Epub 2010 Dec 31.
The purpose of this study was to evaluate the relationship between myocardial strain and coronary flow reserve (CFR) in the prediction of myocardial functional recovery after acute myocardial infarction (AMI).
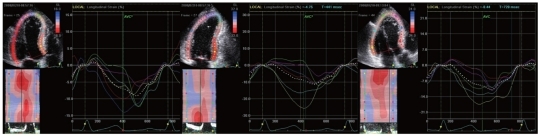
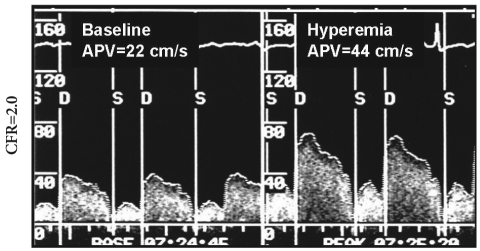
Consecutive patients with anterior ST elevation AMI were analyzed. Left ventricular (LV) strain, determined by 2-dimensional speckle tracking imaging and CFR, determined by intracoronary flow measurement, were obtained on the same day, 3-5 days after primary percutaneous coronary intervention. A-strain was defined as the mean systolic longitudinal strain of 11 LV segments (out of 18) assumed to be supplied by the left anterior descending coronary artery (LAD). Functional recovery was defined as improved wall motion >1 grade seen in at least 2 contiguous dysfunctional segments by echocardiography at the 6-month follow-up.
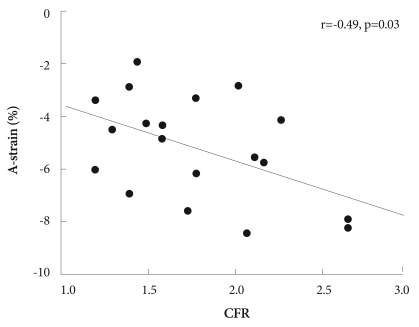
Of 20 patients, 8 patients had preserved CFR (>2.0) and 12 patients had impaired CFR (≤2.0). There were no differences between the 2 CFR groups in LV ejection fractions and wall motion score indices in the LAD territory. However, A-strain was greater in patients with preserved CFR than in patients with impaired CFR (-6.4±2.0% vs. -4.6±1.4%, p=0.03). A-strain and CFR correlated well with each other (r=-0.49, p=0.03). Ten of 20 patients showed functional recovery at 6 months. Of clinical and echocardiographic parameters, A-strain was the only predictor of recovery (odds ratio 2.02, 95% confidence interval=1.03-3.97, p=0.04). For predicting recovery, the sensitivity and specificity were 80.0% and 80.0%, respectively, for CFR (cutoff=1.60), and 60.0% and 90.0%, respectively, for A-strain (cutoff=-6.13%).
Myocardial strain correlates well with the extent of microvascular integrity and can be used as a noninvasive method for predicting recovery after AMI.
本研究旨在评估心肌应变与冠状动脉血流储备(CFR)在预测急性心肌梗死(AMI)后心肌功能恢复中的关系。
对连续的前壁 ST 段抬高 AMI 患者进行分析。在首次经皮冠状动脉介入治疗后 3-5 天,通过二维斑点追踪成像获得左心室(LV)应变,通过冠状动脉内血流测量获得 CFR。A 应变定义为左前降支(LAD)供应的 11 个 LV 节段(18 个节段中的 11 个)的平均收缩期纵向应变。功能恢复定义为超声心动图在 6 个月随访时至少 2 个连续功能障碍节段的壁运动改善>1 级。
20 例患者中,8 例患者 CFR 正常(>2.0),12 例患者 CFR 异常(≤2.0)。2 组 CFR 患者在 LAD 区域的 LV 射血分数和壁运动评分指数方面无差异。然而,CFR 正常组的 A 应变大于 CFR 异常组(-6.4±2.0% vs. -4.6±1.4%,p=0.03)。A 应变与 CFR 之间相关性良好(r=-0.49,p=0.03)。20 例患者中有 10 例在 6 个月时出现功能恢复。在临床和超声心动图参数中,A 应变是恢复的唯一预测因子(优势比 2.02,95%置信区间=1.03-3.97,p=0.04)。对于预测恢复,CFR 的敏感性和特异性分别为 80.0%和 80.0%(截断值=1.60),A 应变分别为 60.0%和 90.0%(截断值=-6.13%)。
心肌应变与微血管完整性程度密切相关,可作为预测 AMI 后恢复的非侵入性方法。