School of Health and Population Sciences, University of Birmingham, Edgbaston, West Midlands B15 2TT, UK.
BMJ. 2011 Feb 3;342:d199. doi: 10.1136/bmj.d199.
To independently evaluate the impact of the second phase of the Health Foundation's Safer Patients Initiative (SPI2) on a range of patient safety measures. Design A controlled before and after design. Five substudies: survey of staff attitudes; review of case notes from high risk (respiratory) patients in medical wards; review of case notes from surgical patients; indirect evaluation of hand hygiene by measuring hospital use of handwashing materials; measurement of outcomes (adverse events, mortality among high risk patients admitted to medical wards, patients' satisfaction, mortality in intensive care, rates of hospital acquired infection). Setting NHS hospitals in England.
Nine hospitals participating in SPI2 and nine matched control hospitals.
The SPI2 intervention was similar to the SPI1, with somewhat modified goals, a slightly longer intervention period, and a smaller budget per hospital.
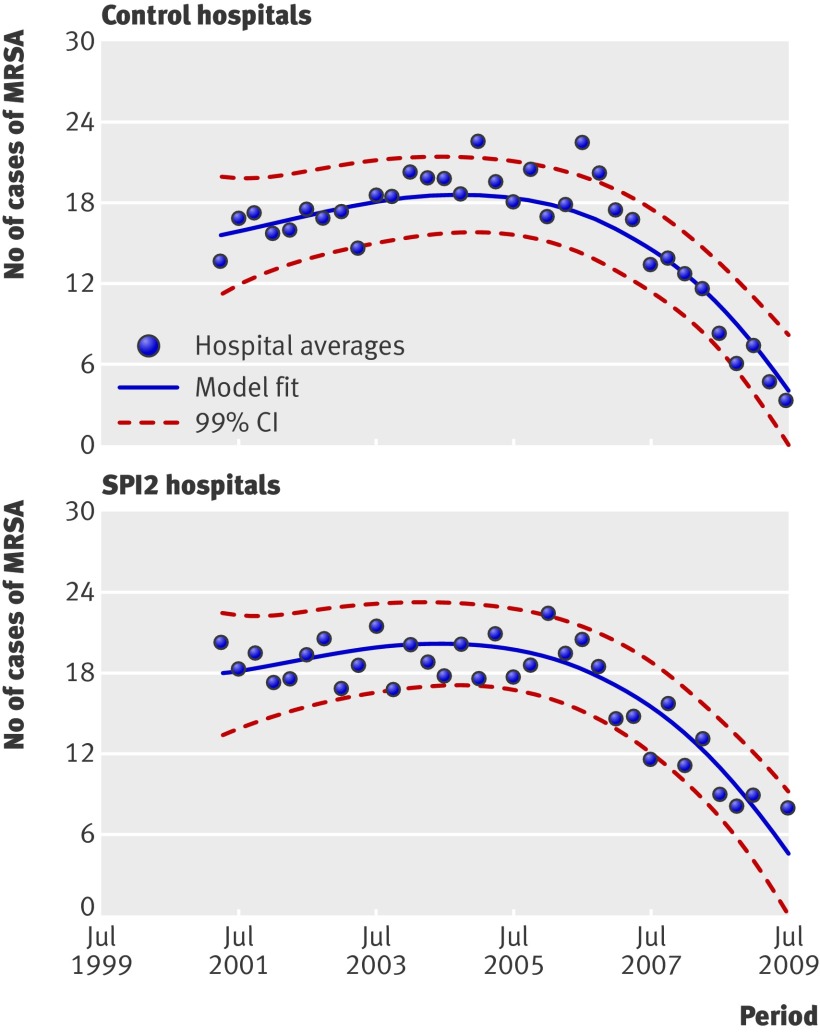
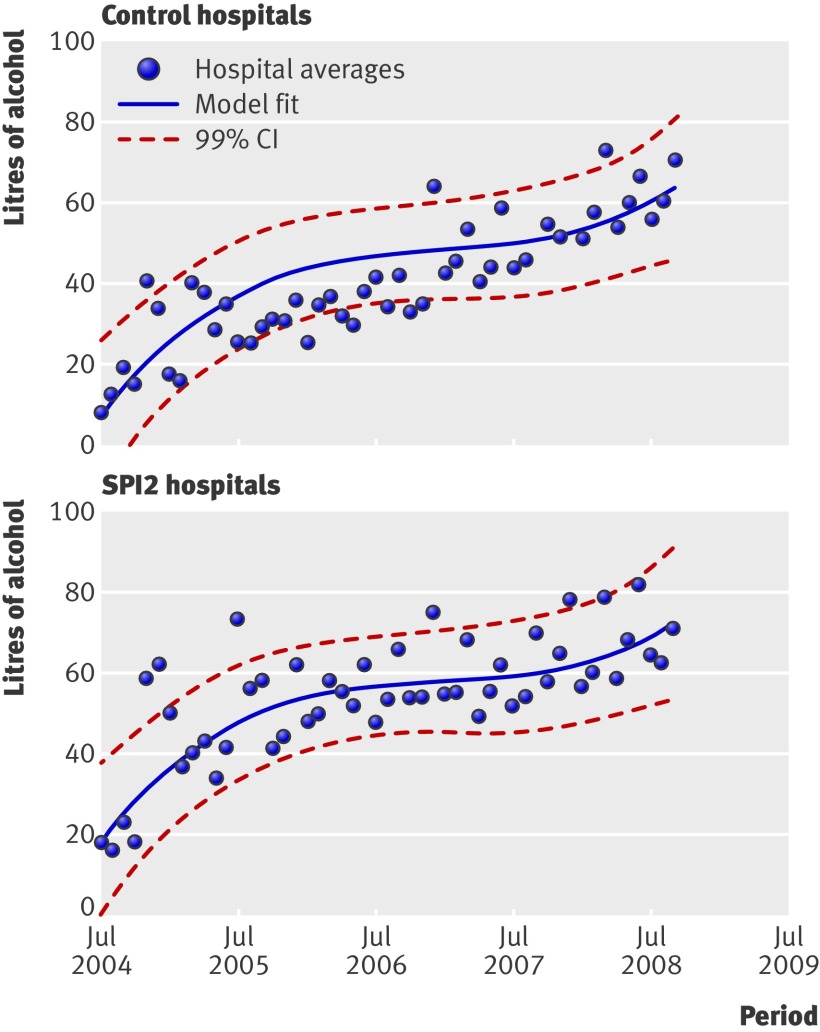
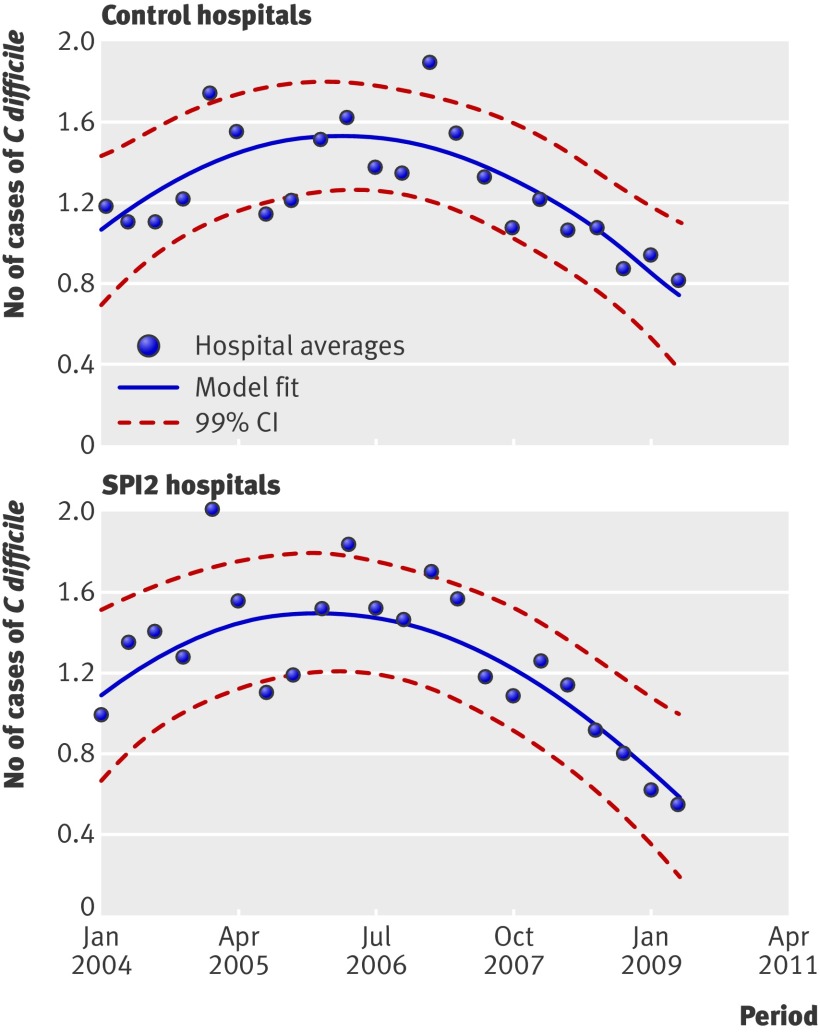
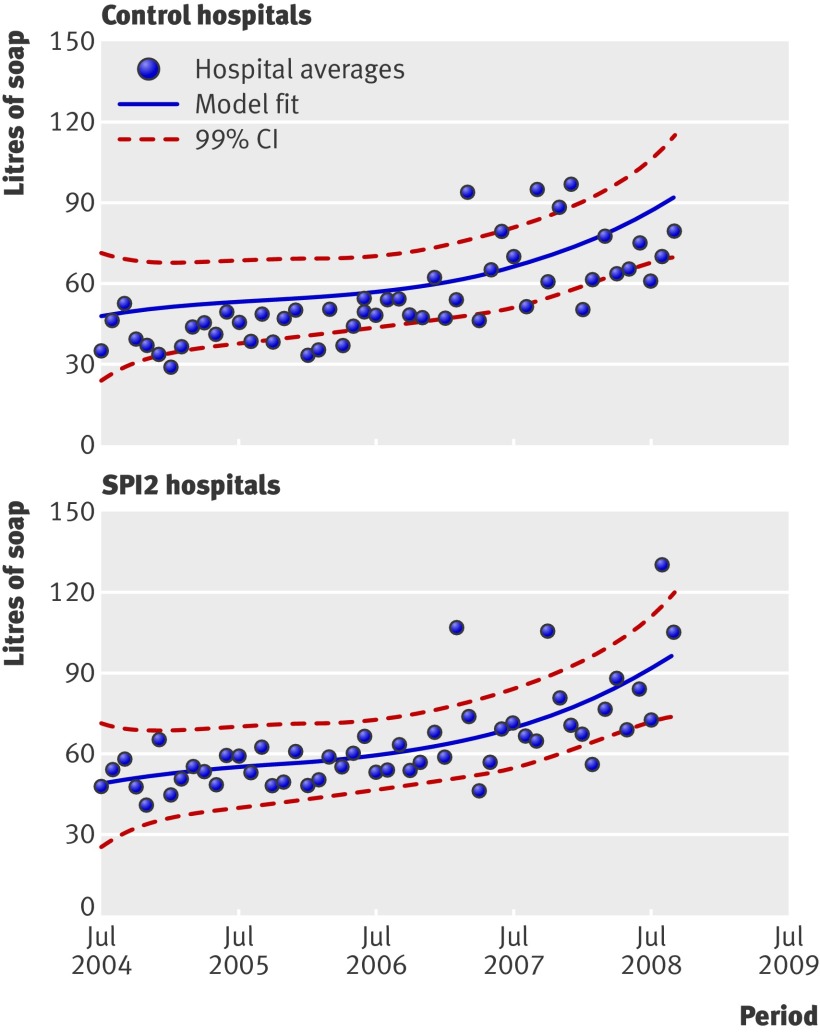
One of the scores (organisational climate) showed a significant (P = 0.009) difference in rate of change over time, which favoured the control hospitals, though the difference was only 0.07 points on a five point scale. Results of the explicit case note reviews of high risk medical patients showed that certain practices improved over time in both control and SPI2 hospitals (and none deteriorated), but there were no significant differences between control and SPI2 hospitals. Monitoring of vital signs improved across control and SPI2 sites. This temporal effect was significant for monitoring the respiratory rate at both the six hour (adjusted odds ratio 2.1, 99% confidence interval 1.0 to 4.3; P = 0.010) and 12 hour (2.4, 1.1 to 5.0; P = 0.002) periods after admission. There was no significant effect of SPI for any of the measures of vital signs. Use of a recommended system for scoring the severity of pneumonia improved from 1.9% (1/52) to 21.4% (12/56) of control and from 2.0% (1/50) to 41.7% (25/60) of SPI2 patients. This temporal change was significant (7.3, 1.4 to 37.7; P = 0.002), but the difference in difference was not significant (2.1, 0.4 to 11.1; P = 0.236). There were no notable or significant changes in the pattern of prescribing errors, either over time or between control and SPI2 hospitals. Two items of medical history taking (exercise tolerance and occupation) showed significant improvement over time, across both control and SPI2 hospitals, but no additional SPI2 effect. The holistic review showed no significant changes in error rates either over time or between control and SPI2 hospitals. The explicit case note review of perioperative care showed that adherence rates for two of the four perioperative standards targeted by SPI2 were already good at baseline, exceeding 94% for antibiotic prophylaxis and 98% for deep vein thrombosis prophylaxis. Intraoperative monitoring of temperature improved over time in both groups, but this was not significant (1.8, 0.4 to 7.6; P = 0.279), and there were no additional effects of SPI2. A dramatic rise in consumption of soap and alcohol hand rub was similar in control and SPI2 hospitals (P = 0.760 and P = 0.889, respectively), as was the corresponding decrease in rates of Clostridium difficile and meticillin resistant Staphylococcus aureus infection (P = 0.652 and P = 0.693, respectively). Mortality rates of medical patients included in the case note reviews in control hospitals increased from 17.3% (42/243) to 21.4% (24/112), while in SPI2 hospitals they fell from 10.3% (24/233) to 6.1% (7/114) (P = 0.043). Fewer than 8% of deaths were classed as avoidable; changes in proportions could not explain the divergence of overall death rates between control and SPI2 hospitals. There was no significant difference in the rate of change in mortality in intensive care. Patients' satisfaction improved in both control and SPI2 hospitals on all dimensions, but again there were no significant changes between the two groups of hospitals.
Many aspects of care are already good or improving across the NHS in England, suggesting considerable improvements in quality across the board. These improvements are probably due to contemporaneous policy activities relating to patient safety, including those with features similar to the SPI, and the emergence of professional consensus on some clinical processes. This phenomenon might have attenuated the incremental effect of the SPI, making it difficult to detect. Alternatively, the full impact of the SPI might be observable only in the longer term. The conclusion of this study could have been different if concurrent controls had not been used.
独立评估健康基金会更安全患者倡议(SPI2)第二阶段对一系列患者安全措施的影响。
前后对照设计的对照试验。
员工态度调查;高危(呼吸)患者在医疗病房的病历回顾;外科患者病历回顾;通过测量医院使用洗手材料间接评估手部卫生;测量结果(不良事件、医疗病房高危患者死亡率、患者满意度、重症监护死亡率、医院获得性感染率)。
英格兰的 NHS 医院。
参与 SPI2 的 9 家医院和 9 家匹配的对照组医院。
SPI2 干预措施与 SPI1 相似,目标略有修改,干预期略长,每家医院的预算略低。
其中一项评分(组织氛围)显示出随着时间的推移,变化率有显著差异(P=0.009),这有利于对照组医院,尽管差异仅为 5 分制的 0.07 分。对高危医疗患者的明确病历回顾显示,在对照组和 SPI2 医院中,某些做法随着时间的推移有所改善(没有恶化的情况),但对照组和 SPI2 医院之间没有显著差异。对照组和 SPI2 站点的生命体征监测都有所改善。这种时间效应在入院后 6 小时(调整后的优势比 2.1,99%置信区间 1.0 至 4.3;P=0.010)和 12 小时(2.4,1.1 至 5.0;P=0.002)时监测呼吸频率方面具有显著意义。SPI 对所有生命体征测量均无显著效果。建议的肺炎严重程度评分系统的使用率从对照组的 1.9%(52/2728)提高到 21.4%(12/56),SPI2 组从 2.0%(50/2506)提高到 41.7%(25/60)。这种时间变化具有显著意义(7.3,1.4 至 37.7;P=0.002),但差异无统计学意义(2.1,0.4 至 11.1;P=0.236)。对照组和 SPI2 医院的处方错误模式没有明显或显著变化。两项病史采集项目(运动耐量和职业)在对照组和 SPI2 医院均随着时间的推移有显著改善,但 SPI2 没有额外的效果。整体评估显示,无论是在时间上还是在对照组和 SPI2 医院之间,错误率都没有显著变化。围手术期护理的明确病历回顾显示,SPI2 针对的四项围手术期标准中的两项的依从率已经很好,抗生素预防的依从率超过 94%,深静脉血栓预防的依从率超过 98%。两组的术中体温监测均随着时间的推移有所改善,但无统计学意义(1.8,0.4 至 7.6;P=0.279),且 SPI2 没有额外的效果。对照组和 SPI2 医院的肥皂和酒精擦手液的使用量都急剧增加(P=0.760 和 P=0.889),艰难梭菌和耐甲氧西林金黄色葡萄球菌感染率也相应下降(P=0.652 和 P=0.693)。对照组病历回顾中纳入的医疗患者的死亡率从 17.3%(42/243)上升到 21.4%(24/112),而 SPI2 医院的死亡率从 10.3%(24/233)下降到 6.1%(7/114)(P=0.043)。不到 8%的死亡被归类为可避免的;死亡率的变化不能解释对照组和 SPI2 医院之间总体死亡率的差异。重症监护病房死亡率的变化率没有显著差异。对照组和 SPI2 医院的患者满意度在所有维度都有所提高,但两组之间没有显著变化。
英格兰 NHS 的许多护理方面已经很好或正在改善,这表明整体质量有了很大的提高。这些改进可能是由于与患者安全相关的同期政策活动,包括与 SPI 具有相似特征的活动,以及一些临床过程的专业共识的出现。这种现象可能削弱了 SPI 的增量效应,使其难以检测到。或者,SPI 的全部影响可能只有在更长的时间内才能显现。如果没有使用同期对照,本研究的结论可能会有所不同。