Department of Hematology and Hematopoietic Cell Transplantation, City of Hope, Duarte, CA 91010, USA.
Bone Marrow Transplant. 2012 Jan;47(1):65-72. doi: 10.1038/bmt.2011.16. Epub 2011 Feb 28.
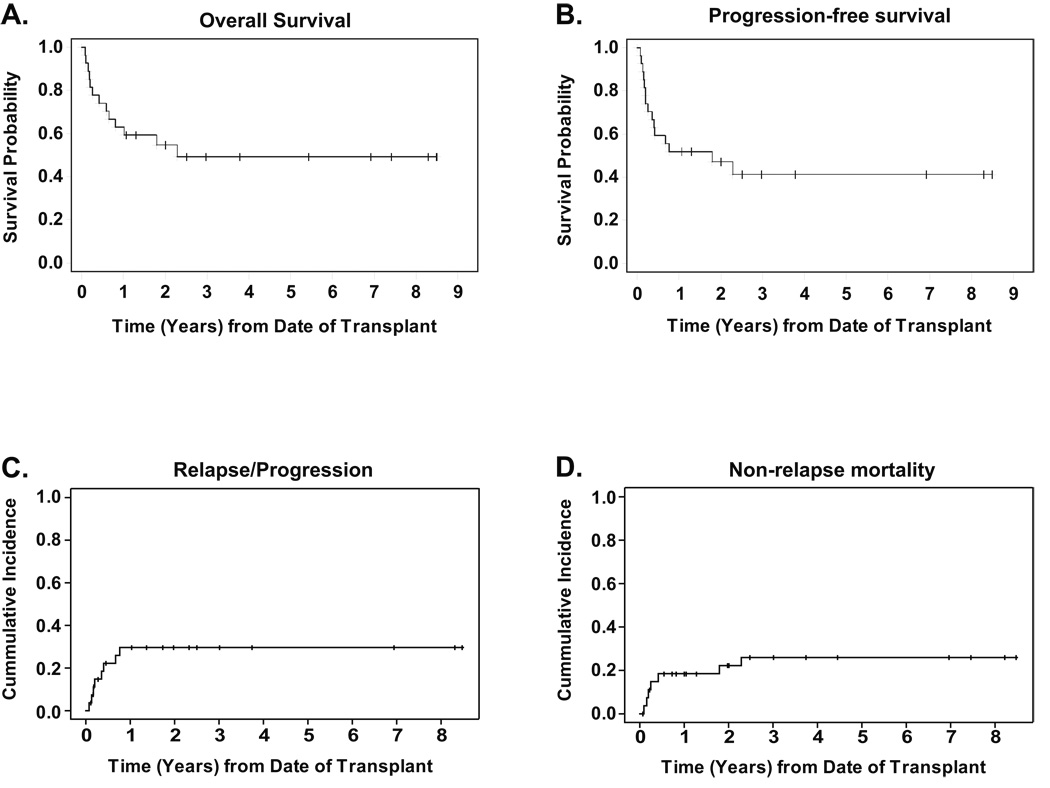
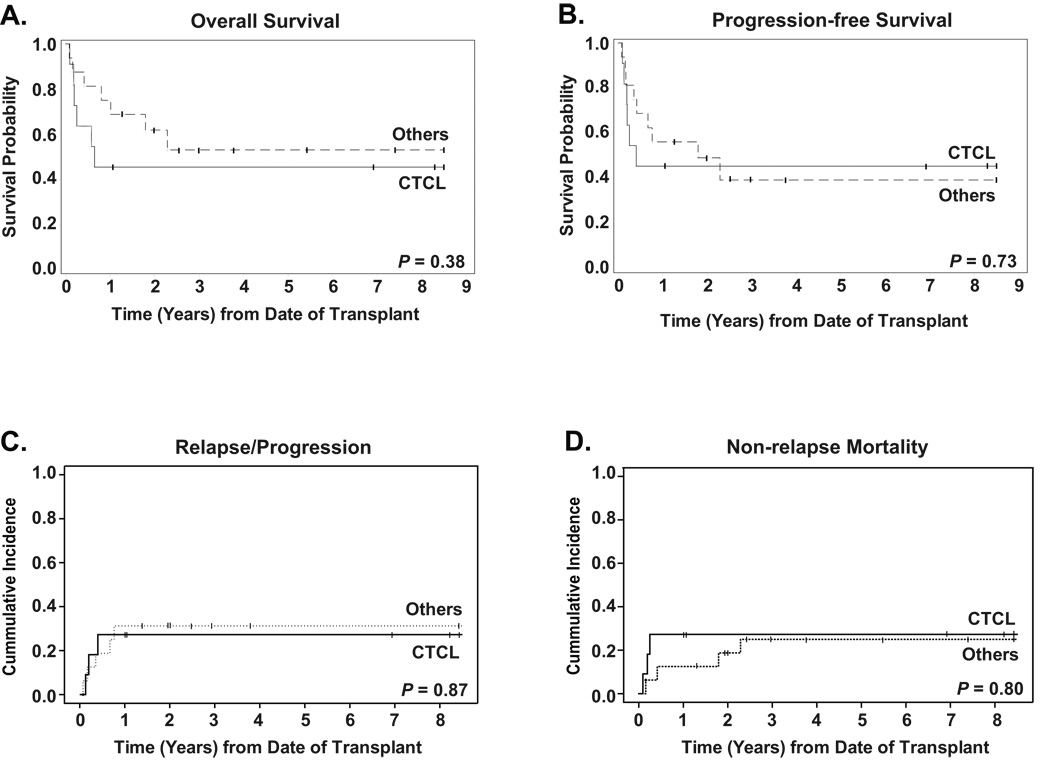
Among non-Hodgkin's lymphoma subtypes, T-cell phenotype confers a poor clinical prognosis. For more aggressive histologies, patients frequently present with advanced disease that is inherently chemoresistant. For cutaneous histologies, disease progresses less rapidly, but is debilitating and often incurable in the long term. Here we report the retrospective analysis of data from 27 patients with mature T-cell lymphoma treated with salvage allogeneic haematopoietic cell transplantation at the City of Hope, Duarte, CA, USA, using a reduced-intensity fludarabine/melphalan conditioning regimen between the years 2001 and 2008. Eleven of the twenty-seven patients had cutaneous T-cell lymphoma (CTCL). The majority of patients had advanced disease at the time of transplant (17/27 or 63%). Median follow-up was 36 months. We observed a 2-year OS of 55%, a PFS of 47% and a cumulative incidence of relapse/progression and non-relapse mortality (NRM) of 30 and 22%, respectively. For CTCL, patients had a 2-year PFS of 45% and NRM of 27% compared with patients with other histologies, who had a PFS of 62% and NRM of 19%. Overall, our results suggest that meaningful long-term survival rates and disease control can be achieved with acceptable non-relapse mortality in patients with mature T-cell lymphomas, including CTCL using reduced-intensity conditioning with melphalan and fludarabine.
在非霍奇金淋巴瘤亚型中,T 细胞表型预示着不良的临床预后。对于更具侵袭性的组织学类型,患者通常表现为进展期疾病,具有内在的化疗耐药性。对于皮肤组织学类型,疾病进展较慢,但长期来看会导致身体虚弱,且通常无法治愈。在这里,我们报告了 27 例成熟 T 细胞淋巴瘤患者的数据回顾性分析,这些患者在加利福尼亚州达勒姆市希望之城接受了挽救性同种异体造血细胞移植,使用了 2001 年至 2008 年期间的低强度氟达拉滨/马法兰预处理方案。27 例患者中有 11 例患有皮肤 T 细胞淋巴瘤(CTCL)。大多数患者在移植时患有晚期疾病(17/27,63%)。中位随访时间为 36 个月。我们观察到 2 年 OS 为 55%,PFS 为 47%,复发/进展和非复发死亡率(NRM)的累积发生率分别为 30%和 22%。对于 CTCL,患者的 2 年 PFS 为 45%,NRM 为 27%,而其他组织学类型的患者 PFS 为 62%,NRM 为 19%。总的来说,我们的结果表明,对于成熟 T 细胞淋巴瘤患者,包括使用马法兰和氟达拉滨进行低强度预处理的 CTCL,采用低强度预处理方案进行挽救性同种异体造血细胞移植,可以实现有意义的长期生存率和疾病控制,同时接受可接受的非复发死亡率。