Samra Tanvir, Pawar Mridula, Yadav Amlendu
Department of Anesthesia and Intensive Care, Dr. Ram Manohar Lohia Hospital, Connaught Place, New Delhi, India.
Indian J Anaesth. 2011 Jan;55(1):47-51. doi: 10.4103/0019-5049.76602.
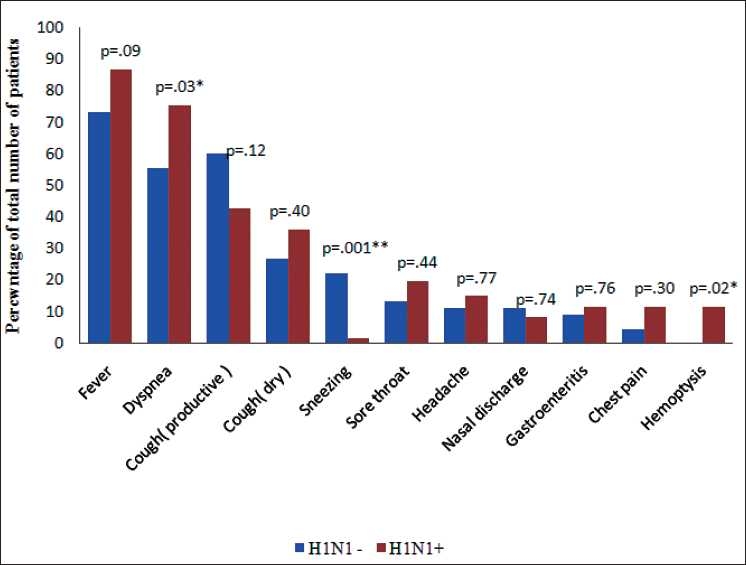
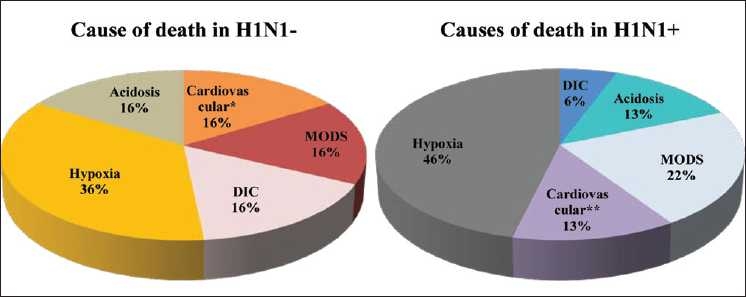
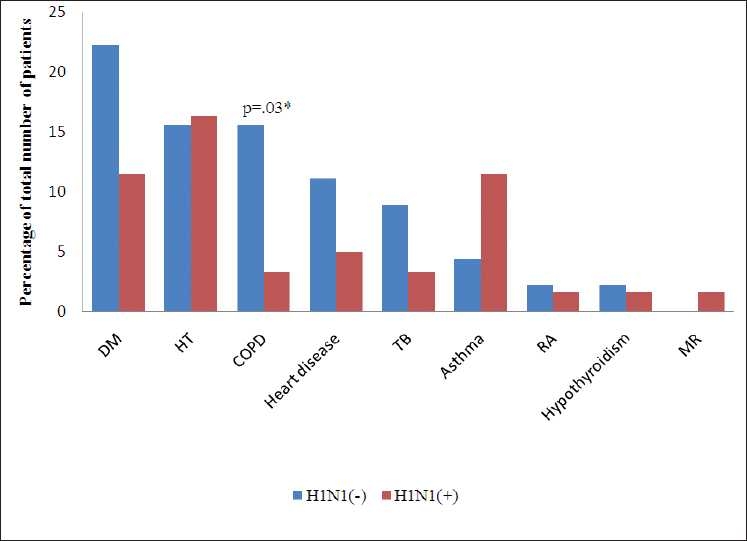
H1N1 subtype of influenza A virus has clinical presentation ranging from mild flu like illness to severe lung injury and acute respiratory distress syndrome (ARDS). The aim of our study was to compare the demographic characteristics, clinical presentation, and mortality of critically ill patients with (H1N1+) and without H1N1 infection (H1N1-). We retrospectively analyzed medical charts of patients admitted in "Swine Flu ICU" with ARDS from August 2009 to May 2010. Real-time reverse transcriptase polymerase chain reaction (RT-PCR) assay was used for detection of H1N1 virus in the respiratory specimens. Clinical data from 106 (H1N1, 45; H1N1+, 61) patients was collected and compared. Mean delay in presentation to our hospital was 5.7 ± 3.1 days and co-morbidities were present in two-fifth of the total admissions. Sequential Organ Failure Assessment (SOFA) score of patients with and without H1N1 infection was comparable; 7.8 ± 3.5 and 6.6 ± 3.1 on day 1 and 7.2 ± 4.5 and 6.5 ± 3.1 on day 3, respectively. H1N1+ patients were relatively younger in age (34.2 ± 12.9 years vs. 42.8 ± 18.1, P = 0.005) but presented with significantly lower PaO(2):FiO(2) ratio (87.3 ± 48.7 vs. 114 ± 51.7) in comparison to those who subsequently tested as H1N1. The total leucocyte counts were significantly lower in H1N1+ patients during the first four days of illness but incidence of renal failure (P = 0.02) was higher in H1N1+ patients. The mortality in both the groups was high (H1N1+, 77%; H1N1, 68%) but comparable. There was a mean delay of 5.7 ± 3.1 days in initiation of antivirals. Patients with H1N1 infection were relatively younger in age and with a significantly higher incidence of refractory hypoxia and acute renal failure. Mortality from ARDS reported in our study in both the groups was high but comparable.
甲型流感病毒H1N1亚型的临床表现从类似流感的轻症到严重肺损伤及急性呼吸窘迫综合征(ARDS)不等。我们研究的目的是比较患有H1N1感染(H1N1+)和未感染H1N1(H1N1-)的危重症患者的人口统计学特征、临床表现及死亡率。我们回顾性分析了2009年8月至2010年5月入住“猪流感重症监护病房”且患有ARDS的患者的病历。采用实时逆转录聚合酶链反应(RT-PCR)检测法检测呼吸道标本中的H1N1病毒。收集并比较了106例患者(H1N1,45例;H1N1+,61例)的临床数据。患者到我院就诊的平均延迟时间为5.7±3.1天,五分之二的入院患者存在合并症。H1N1感染患者和未感染患者的序贯器官衰竭评估(SOFA)评分具有可比性;第1天分别为7.8±3.5和6.6±3.1,第3天分别为7.2±4.5和6.5±3.1。H1N1+患者年龄相对较小(34.2±12.9岁对42.8±18.1岁,P = 0.005),但与后来检测为H1N1阴性的患者相比,其动脉血氧分压与吸入氧浓度比值(PaO₂:FiO₂)显著更低(87.3±48.7对114±51.7)。H1N1+患者在发病的前四天白细胞总数显著更低,但H1N1+患者肾衰竭的发生率更高(P = 0.02)。两组的死亡率都很高(H1N1+,77%;H1N1-,68%),但具有可比性。抗病毒药物开始使用的平均延迟时间为5.7±3.1天。H1N1感染患者年龄相对较小,难治性低氧血症和急性肾衰竭的发生率显著更高。我们研究中报告的两组ARDS死亡率都很高,但具有可比性。