Hong Seung-Dok, Kim Yeo-Kyeoung, Kim Hee-Nam, Lee Se Ryeon, Ahn Jae-Sook, Yang Deok-Hwan, Lee Je-Jung, Lee Il-Kwon, Shin Myung-Geun, Kim Hyeoung-Joon
Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea.
Korean J Hematol. 2011 Mar;46(1):24-30. doi: 10.5045/kjh.2011.46.1.24. Epub 2011 Mar 15.
All-trans retinoic acid (ATRA)/anthracycline chemotherapy is beneficial in newly diagnosed acute promyelocytic leukemia (APL); however, it is important to identify patients with high-risk disease to increase the cure rate. We investigated the outcome of ATRA/anthracycline chemotherapy and clinicobiological correlations of FLT3/ITD and NPM1 mutations in APL patients.
Induction therapy included oral ATRA (45 mg/m(2)/day) and idarubicin (12 mg/m(2)/day, intravenous, on days 2, 4, and 6). Patients achieving complete remission (CR) received 3 courses of ATRA combined with reinforced consolidation therapy. Mutations were analyzed using GeneScan and polymerasae chain reaction assays of bone marrow samples obtained from patients at diagnosis.
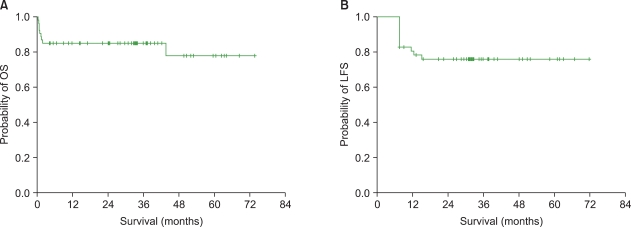
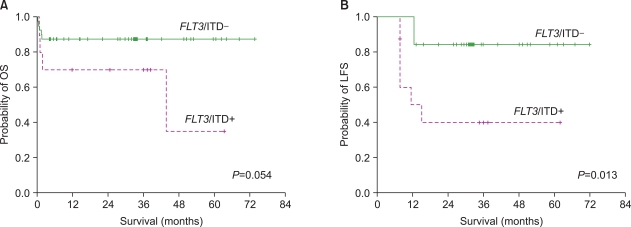
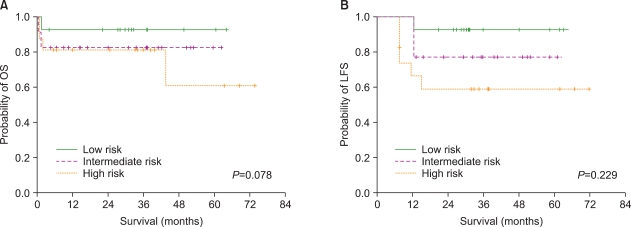
Forty-five (84.9%) of 53 eligible patients achieved CR. The overall relapse rate was 8.9%, and the 3-year overall survival (OS) and leukemia-free survival (LFS) were 84.9±4.9% and 77.5±6.0%, respectively. The NPM1 mutation was not found in any patient, while the FLT3/ITD mutation was found in 10 (20.0%) patients. Of the FLT3/ITD+ patients, 80% belonged to the high-risk group, defined according to the presenting WBC and platelet counts. Among the patients who achieved CR, those who were FLT3/ITD+ had a higher relapse rate than those FLT3/ITD-. FLT3/ITD+ patients also had a significantly lower 3-year LFS than FLT3/ITD- patients. Multivariate analysis of the LFS showed that the FLT3/ITD mutation was independently associated with a shorter overall LFS, after adjusting for pretreatment risk stratification.
This study investigated the clinical outcome of newly diagnosed APL patients treated with ATRA/anthracycline chemotherapy. Patients carrying the FLT3/ITD mutation had more aggressive clinical features and a poorer clinical outcome.
全反式维甲酸(ATRA)/蒽环类化疗对新诊断的急性早幼粒细胞白血病(APL)有益;然而,识别高危疾病患者以提高治愈率很重要。我们研究了APL患者中ATRA/蒽环类化疗的结果以及FLT3/ITD和NPM1突变的临床生物学相关性。
诱导治疗包括口服ATRA(45mg/m²/天)和伊达比星(12mg/m²/天,静脉注射,第2、4和6天)。达到完全缓解(CR)的患者接受3个疗程的ATRA联合强化巩固治疗。使用基因扫描和聚合酶链反应分析诊断时从患者获得的骨髓样本中的突变。
53例符合条件的患者中有45例(84.9%)达到CR。总复发率为8.9%,3年总生存率(OS)和无白血病生存率(LFS)分别为84.9±4.9%和77.5±6.0%。未在任何患者中发现NPM1突变,而在10例(20.0%)患者中发现FLT3/ITD突变。在FLT3/ITD+患者中,80%属于根据初诊时白细胞和血小板计数定义的高危组。在达到CR的患者中,FLT3/ITD+患者的复发率高于FLT3/ITD-患者。FLT3/ITD+患者的3年LFS也显著低于FLT3/ITD-患者。LFS的多变量分析表明,在调整预处理风险分层后,FLT3/ITD突变与总体LFS缩短独立相关。
本研究调查了新诊断的接受ATRA/蒽环类化疗的APL患者的临床结果。携带FLT3/ITD突变的患者具有更具侵袭性的临床特征和更差的临床结果。