Division of Medical Oncology B, Regina Elena National Cancer Institute, Rome, Italy.
J Exp Clin Cancer Res. 2011 Apr 12;30(1):39. doi: 10.1186/1756-9966-30-39.
To evaluate activity and tolerability of two anthracycline-containing regimens as first-line treatment for anthracycline-naïve relapsed breast cancer patients.
Patients with relapsed breast cancer not previously treated with adjuvant anthracyclines were randomly assigned to epirubicin/vinorelbine (arm A: EPI/VNB, EPI 90 mg/m2 on day 1, VNB 25 mg/m2 on days 1,5 plus G-CSF subcutaneously on days 7-12, with cycles repeated every 21 days), or to pegylated liposomal doxorubicin/VNB (arm B: PLD/VNB, PLD 40 mg/m2 on day 1, VNB 30 mg/m2 on days 1, 15, with cycles repeated every 4 weeks). Primary objective was to evaluate the efficacy of the two regimens in terms of response rate, secondarily toxicity, progression free survival and overall survival.
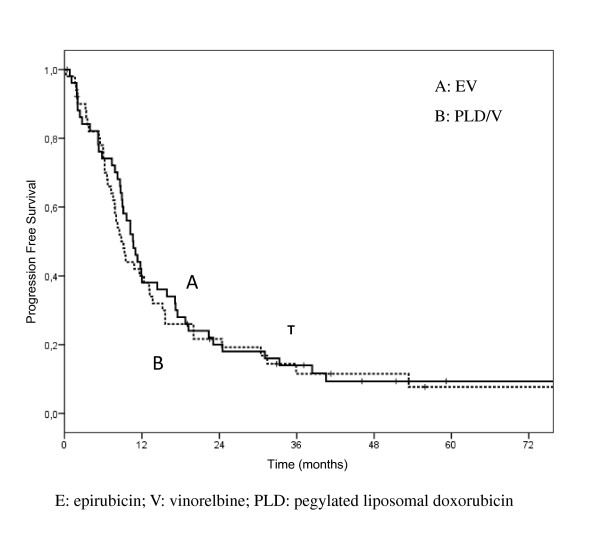
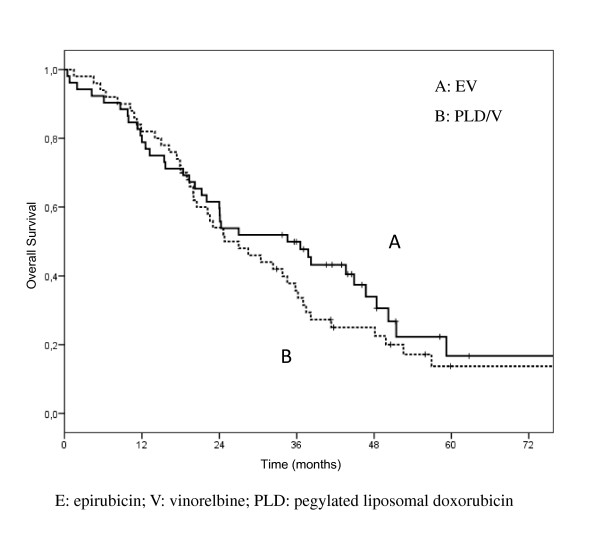
One hundred and four patients have been enrolled (arm A 54, arm B 50): characteristics were well balanced between the 2 arms. Responses were as follows: arm A, 3 (5.6%) CR, 20 (37%) PR, (ORR 42.6%, 95%CI 29.3%-55.9%); arm B, 8 (16%) CR, 18 (36%) PR, (ORR 52%, 95%CI 38.2%-65.8%). Median progression free survival was 10.7 months in arm A (95% CI, 8.7-12.6), and 8.8 months in arm B (95% CI, 7.1-10.5). Median overall survival was 34.6 months in arm A (95%CI, 19.5-49.8) and 24.8 months in arm B (95%CI, 15.7-33.9). As toxicity concerns, both treatment regimens were well tolerated; myelosuppression was the dose-limiting toxicity, with G3-4 neutropenia occurring in 18.5% and 22% of the patients of arm A and B, respectively. No relevant differences in main toxic effects have been observed between the two arms, except for alopecia, more common in arm A, and cutaneous toxicity, observed only in arm B. No clinical congestive heart failures have been observed, one case of tachyarrhythmia was reported after the last EPI/VNB cycle, and two reversible ≥ 20% LVEF decreases have been observed in arm A.
Both anthracycline- containing regimens evaluated in the present study seem to be active and with a satisfactory tolerability in anthracycline-naïve relapsed breast cancer patients.
评估两种含蒽环类药物的方案作为蒽环类药物初治复发乳腺癌患者的一线治疗的疗效和耐受性。
既往未接受辅助蒽环类药物治疗的复发乳腺癌患者被随机分配接受表柔比星/长春瑞滨(A 组:EPI/VNB,EPI90mg/m2 第 1 天,VNB25mg/m2 第 1、5 天,同时皮下给予 G-CSF 第 7-12 天,每 21 天重复一个周期)或聚乙二醇化脂质体多柔比星/长春瑞滨(B 组:PLD/VNB,PLD40mg/m2 第 1 天,VNB30mg/m2 第 1、15 天,每 4 周重复一个周期)。主要目的是评估两种方案在缓解率、次要毒性、无进展生存期和总生存期方面的疗效。
共纳入 104 例患者(A 组 54 例,B 组 50 例):两组之间的特征平衡良好。反应如下:A 组,3 例(5.6%)完全缓解,20 例(37%)部分缓解,总缓解率为 42.6%(95%CI29.3%-55.9%);B 组,8 例(16%)完全缓解,18 例(36%)部分缓解,总缓解率为 52%(95%CI38.2%-65.8%)。A 组无进展生存期中位数为 10.7 个月(95%CI8.7-12.6),B 组为 8.8 个月(95%CI7.1-10.5)。A 组总生存期中位数为 34.6 个月(95%CI19.5-49.8),B 组为 24.8 个月(95%CI15.7-33.9)。在毒性方面,两种治疗方案均耐受良好;骨髓抑制是剂量限制毒性,A 组和 B 组分别有 18.5%和 22%的患者发生 3-4 级中性粒细胞减少症。两组之间除脱发(A 组更常见)和皮肤毒性(仅见于 B 组)外,主要毒性作用无明显差异。未观察到与蒽环类药物相关的充血性心力衰竭,EPI/VNB 最后一个周期后报告了 1 例心动过速性心律失常,A 组有 2 例可逆性 LVEF 降低≥20%。
在本研究中评估的两种含蒽环类药物的方案在蒽环类药物初治复发乳腺癌患者中似乎具有活性和良好的耐受性。