Sheps Center for Health Services Research, Universityof North Carolina at Chapel Hill, 725 Martin LutherKing, Jr. Boulevard, Chapel Hill, NC 27599-7590, USA.
Arthritis Care Res (Hoboken). 2011 Jul;63(7):1020-30. doi: 10.1002/acr.20477.
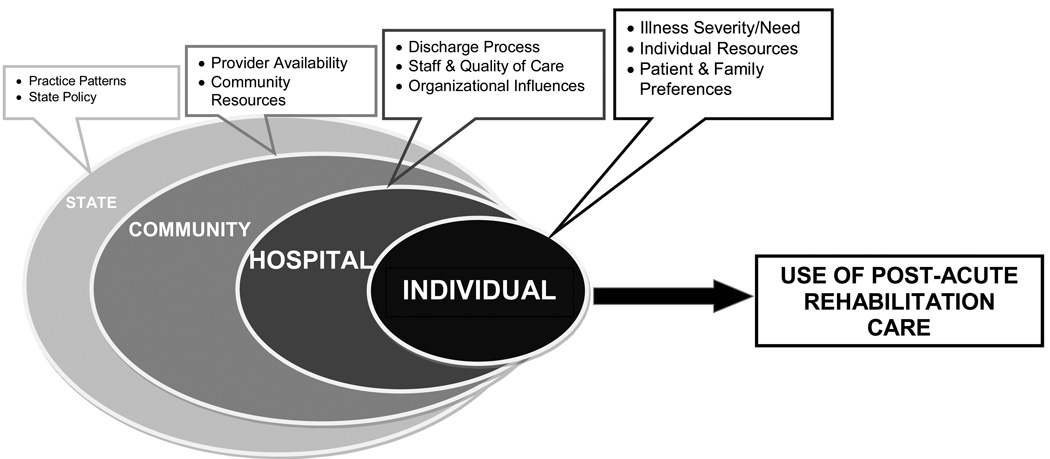
To determine the extent to which demographic and geographic disparities exist in the use of post-acute rehabilitation care (PARC) for joint replacement.
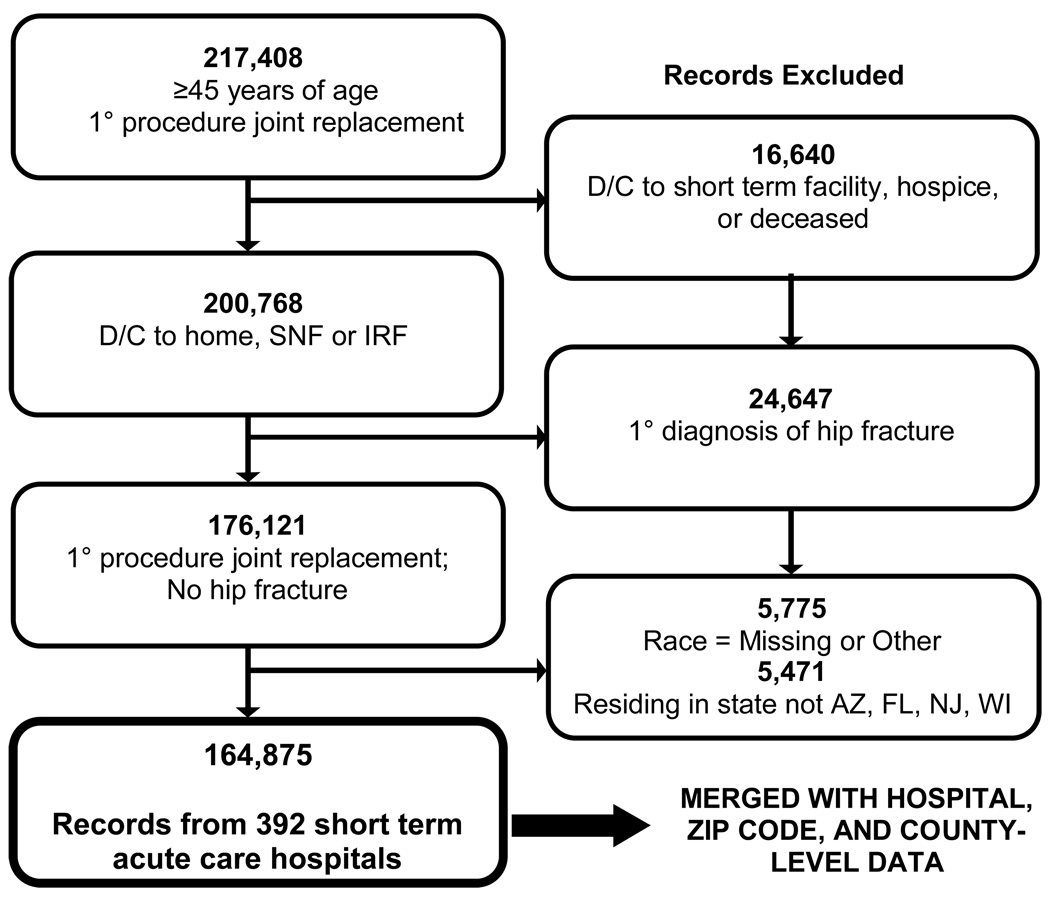
We conducted a cross-sectional analysis of 2 years (2005 and 2006) of population-based hospital discharge data from 392 hospitals in 4 states (Arizona, Florida, New Jersey, and Wisconsin). A total of 164,875 individuals who were age ≥ 45 years, admitted to the hospital for a hip or knee joint replacement, and who survived their inpatient stay were identified. Three dichotomous dependent variables were examined: 1) discharge to home versus institution (i.e., skilled nursing facility [SNF] or inpatient rehabilitation facility [IRF]), 2) discharge to home with versus without home health (HH), and 3) discharge to an SNF versus an IRF. Multilevel logistic regression analyses were conducted to identify demographic and geographic disparities in PARC use, controlling for illness severity/comorbidities, hospital characteristics, and PARC supply. Interactions among race, socioeconomic, and geographic variables were explored.
Considering PARC as a continuum from more to less intensive care in regard to hours of rehabilitation per day (e.g., IRF→SNF→HH→no HH), the uninsured received less intensive care in all 3 models. Individuals receiving Medicaid and those of lower socioeconomic status received less intensive care in the HH versus no HH and SNF versus IRF models. Individuals living in rural areas received less intensive care in the institution versus home and HH versus no HH models. The effect of race was modified by insurance and by state. In most instances, minorities received less intensive care. PARC use varied by hospital.
Efforts to further understand the reasons behind these disparities and their effect on outcomes are needed.
确定在接受关节置换术后康复治疗(PARC)方面,人口统计学和地理差异的程度。
我们对来自 4 个州(亚利桑那州、佛罗里达州、新泽西州和威斯康星州)的 392 家医院的 2 年(2005 年和 2006 年)基于人群的医院出院数据进行了横断面分析。共确定了 164875 名年龄≥45 岁、因髋关节或膝关节置换住院、并在住院期间存活的患者。检查了 3 个二分依赖变量:1)出院回家与出院到机构(即,熟练护理机构[SNF]或住院康复机构[IRF]),2)出院回家伴或不伴家庭健康(HH),3)出院到 SNF 与 IRF。进行多水平逻辑回归分析,以确定 PARC 使用方面的人口统计学和地理差异,同时控制疾病严重程度/合并症、医院特征和 PARC 供应。探讨了种族、社会经济和地理变量之间的相互作用。
考虑到 PARC 作为康复治疗每天小时数(例如,IRF→SNF→HH→无 HH)从更密集到更不密集的护理连续体,在所有 3 个模型中,无保险者接受的护理程度较低。接受医疗补助的人和社会经济地位较低的人在 HH 与无 HH 和 SNF 与 IRF 模型中接受的护理程度较低。居住在农村地区的人在机构与家庭以及 HH 与无 HH 模型中接受的护理程度较低。种族的影响受到保险和州的影响。在大多数情况下,少数民族接受的护理程度较低。PARC 的使用因医院而异。
需要进一步努力了解这些差异背后的原因及其对结果的影响。