Faculty of Health Sciences, University of Ottawa, Ottawa, Ontario, Canada;
Clin Epidemiol. 2011 Mar 28;3:107-29. doi: 10.2147/CLEP.S16235.
Most patients with moderate and severe chronic obstructive pulmonary disease (COPD) receive long-acting bronchodilators (LABA) for symptom control. It is, however, unclear if and what drug treatments should be added to LABAs to reduce exacerbations, which is an important goal of COPD management. Since current guidelines cannot make strong recommendations yet, our aim was to determine the relative efficacy of existing treatments and combinations to reduce the risk for COPD exacerbations.
We included randomized clinical trials (RCTs) evaluating long-acting β(2) agonists (LABA), long-acting muscarinic antagonists (LAMA), inhaled glucocorticosterioids (ICS), and the phosphodiesterase-4 (PDE4) inhibitor roflumilast, and combinations of these interventions in moderate to severe COPD populations. Our primary outcome was the event rate of exacerbations. We conducted a random-effects Bayesian mixed-treatment comparison (MTC) and applied several sensitivity analyses. In particular, we confirmed our findings using a binomial MTC analysis examining whether a patient experienced at least one exacerbation event or not during the trial. We also used an additive assumption to calculate the combined effects of treatments that were not included in the systematic review.
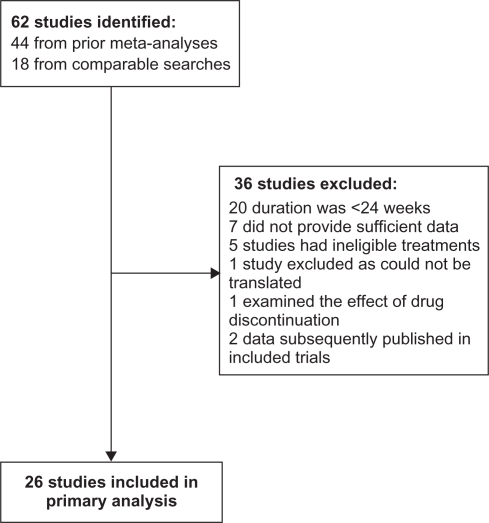
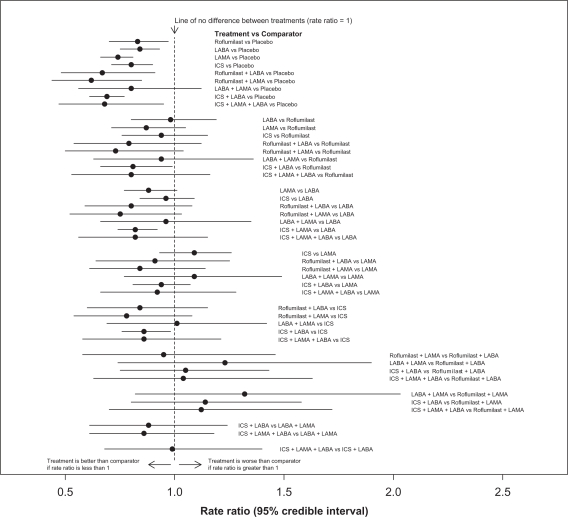
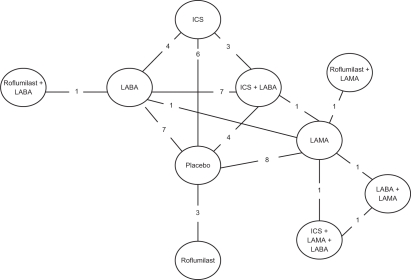
Twenty-six studies provided data on the total number of exacerbations and/or the mean annual rate of exacerbations among a combined 36,312 patients. There were a total of 10 treatment combinations in the MTC and 15 in the additive analysis. Compared with all other treatments, the combination of roflumilast plus LAMA exhibited the largest treatment effects, and had the highest probability (45%) of being the best first-line treatment. This was consistent whether applying the incidence rate analysis or the binomial analysis. When applying the additive assumption, most point estimates suggested that roflumilast may provide additional benefit by further reducing exacerbations.
Using various meta-analytic approaches, our study demonstrates that depending on the choice of drug, combined treatments offer a therapeutic advantage.
大多数中重度慢性阻塞性肺疾病(COPD)患者接受长效支气管扩张剂(LABA)治疗以控制症状。然而,尚不清楚是否以及应添加何种药物治疗以减少COPD 恶化,这是 COPD 管理的重要目标。由于目前的指南尚不能提出强有力的建议,我们的目的是确定现有治疗方法和组合以降低 COPD 恶化风险的相对疗效。
我们纳入了评估长效β(2)激动剂(LABA)、长效毒蕈碱拮抗剂(LAMA)、吸入性糖皮质激素(ICS)和磷酸二酯酶-4(PDE4)抑制剂罗氟司特以及这些干预措施联合应用于中重度 COPD 人群的随机临床试验(RCT)。我们的主要结局是恶化事件的发生率。我们进行了随机效应贝叶斯混合治疗比较(MTC)并进行了几项敏感性分析。特别是,我们使用二项式 MTC 分析检查患者在试验期间是否至少经历过一次恶化事件来确认我们的发现。我们还使用了一个附加假设来计算未包含在系统评价中的治疗的联合效应。
26 项研究提供了有关 36312 例患者的总恶化次数和/或年平均恶化率的数据。MTC 中有 10 种治疗组合,附加分析中有 15 种。与所有其他治疗相比,罗氟司特联合 LAMA 的治疗效果最大,成为最佳一线治疗的可能性最高(45%)。这在应用发生率分析或二项式分析时都是一致的。当应用附加假设时,大多数点估计表明罗氟司特可能通过进一步减少恶化提供额外的益处。
使用各种荟萃分析方法,我们的研究表明,根据药物的选择,联合治疗提供了治疗优势。