Department of Gynecologic Oncology, The University of Texas M. D. Anderson Cancer Center, Houston, Texas 77030, USA.
Cancer. 2011 May 1;117(9):1928-34. doi: 10.1002/cncr.25739. Epub 2010 Nov 16.
Failure to detect metastasis to para-aortic nodes in patients with locally advanced cervical cancer leads to suboptimal treatment. No previous studies have prospectively compared positron emission tomography (PET)/computed tomography (CT) with laparoscopic extraperitoneal staging in the evaluation of para-aortic lymph nodes.
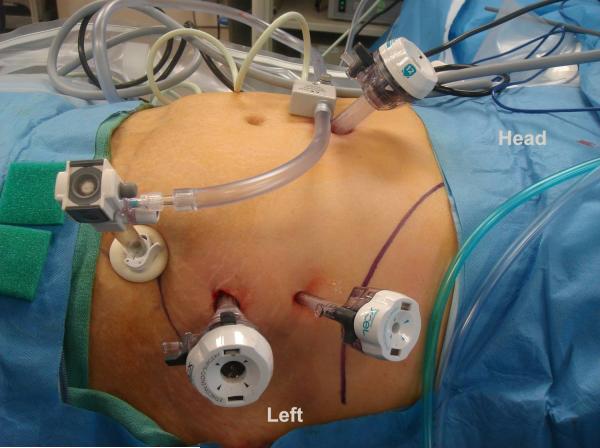
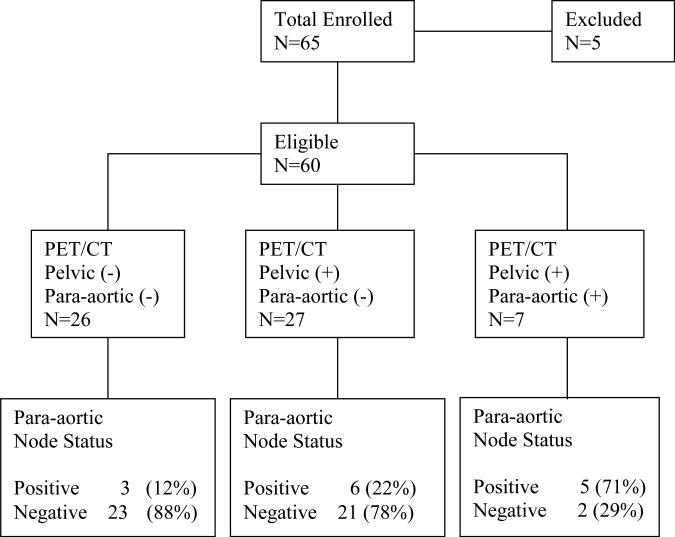
Sixty-five patients were enrolled; 60 were available for analysis. Patients with stage IB2-IVA cervical cancer without evidence of para-aortic lymphadenopathy on preoperative CT or magnetic resonance imaging (MRI) were prospectively enrolled. All patients underwent preoperative PET/CT. Laparoscopic extraperitoneal lymphadenectomy was performed from the common iliac vessels to the left renal vein.
The median age at diagnosis was 48 years (range, 23-84). The median operative time was 140 minutes (range, 89-252). The median blood loss was 22.5 mL (range, 5-150). The median length of hospital stay was 1 day (range, 0-4). The median number of lymph nodes retrieved was 11 (range, 1-39). Fourteen (23%) patients had histopathologically positive para-aortic nodes. Of the 26 patients with negative pelvic and para-aortic nodes on PET/CT, 3 (12%) had histopathologically positive para-aortic nodes. Of the 27 patients with positive pelvic but negative para-aortic nodes on PET/CT, 6 (22%) had histopathologically positive para-aortic nodes. The sensitivity and specificity of PET/CT in detecting positive para-aortic nodes when nodes were negative on CT or MRI were 36% and 96%, respectively. Eleven (18.3%) patients had a treatment modification based on surgical findings.
Laparoscopic extraperitoneal para-aortic lymphadenectomy is safe and feasible. Surgical staging of patients with locally advanced cervical cancer should be considered before planned radiation and chemotherapy.
局部晚期宫颈癌患者如果未能检测到腹主动脉旁淋巴结转移,会导致治疗效果不佳。既往研究均未前瞻性比较正电子发射断层扫描(PET)/计算机断层扫描(CT)与腹腔镜腹膜外分期在评估腹主动脉旁淋巴结中的作用。
共纳入 65 例患者,其中 60 例可供分析。所有患者均为术前 CT 或磁共振成像(MRI)未见腹主动脉旁淋巴结肿大的 IB2 期-IVA 期宫颈癌患者。所有患者均行术前 PET/CT 检查,然后行腹腔镜腹膜外淋巴结切除术,范围从髂总血管至左肾静脉。
中位诊断年龄为 48 岁(范围 23-84 岁),中位手术时间为 140 分钟(范围 89-252 分钟),中位术中出血量为 22.5 毫升(范围 5-150 毫升),中位住院时间为 1 天(范围 0-4 天),中位淋巴结清扫数为 11 枚(范围 1-39 枚)。14 例(23%)患者的腹主动脉旁淋巴结有组织病理学阳性结果。26 例 PET/CT 显示盆腔和腹主动脉旁淋巴结阴性的患者中,有 3 例(12%)存在腹主动脉旁淋巴结组织学阳性。27 例 PET/CT 显示盆腔淋巴结阳性而腹主动脉旁淋巴结阴性的患者中,有 6 例(22%)存在腹主动脉旁淋巴结组织学阳性。当 CT 或 MRI 显示淋巴结阴性时,PET/CT 检测阳性腹主动脉旁淋巴结的敏感性和特异性分别为 36%和 96%。根据手术结果,有 11 例(18.3%)患者的治疗方案发生了改变。
腹腔镜腹膜外腹主动脉旁淋巴结切除术安全可行。对于计划接受放化疗的局部晚期宫颈癌患者,应考虑进行外科分期。