Department of Surgery, University of Florida, Gainesville, Florida, USA.
PLoS One. 2011 Apr 29;6(4):e18890. doi: 10.1371/journal.pone.0018890.
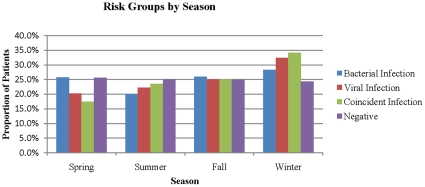
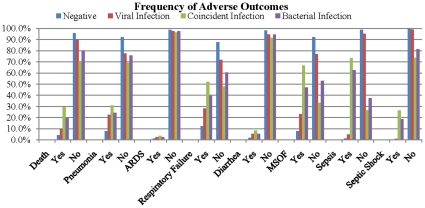
Viruses are the most common source of infection among immunocompetent individuals, yet they are not considered a clinically meaningful risk factor among the critically ill. This work examines the association of viral infections diagnosed during the hospital stay or not documented as present on admission to the outcomes of ICU patients with no evidence of immunosuppression on admission. This is a population-based retrospective cohort study of University HealthSystem Consortium (UHC) academic centers in the U.S. from the years 2006 to 2009. The UHC is an alliance of over 90% of the non-profit academic medical centers in the U.S. A total of 209,695 critically ill patients were used in this analysis. Eight hospital complications were examined. Patients were grouped into four cohorts: absence of infection, bacterial infection only, viral infection only, and bacterial and viral infection during same hospital admission. Viral infections diagnosed during hospitalization significantly increased the risk of all complications. There was also a seasonal pattern for viral infections. Specific viruses associated with poor outcomes included influenza, RSV, CMV, and HSV. Patients who had both viral and bacterial infections during the same hospitalization had the greatest risk of mortality RR 6.58, 95% CI (5.47, 7.91); multi-organ failure RR 8.25, 95% CI (7.50, 9.07); and septic shock RR 271.2, 95% CI (188.0, 391.3). Viral infections may play a significant yet unrecognized role in the outcomes of ICU patients. They may serve as biological markers or play an active role in the development of certain adverse complications by interacting with coincident bacterial infection.
病毒是免疫功能正常个体中最常见的感染源,但在重症患者中,它们并不被认为是具有临床意义的危险因素。本研究旨在探讨住院期间诊断的病毒感染与入院时未记录为存在的病毒感染与无入院时免疫抑制证据的 ICU 患者结局之间的关系。这是一项基于人群的美国大学卫生系统联合会(UHC)学术中心的回顾性队列研究,时间范围为 2006 年至 2009 年。UHC 是美国 90%以上非营利性学术医疗中心的联盟。本分析共使用了 209695 名重症患者。共检查了 8 种医院并发症。患者分为四组:无感染、仅有细菌感染、仅有病毒感染以及同一住院期间发生细菌和病毒感染。住院期间诊断的病毒感染显著增加了所有并发症的风险。病毒感染也存在季节性模式。与不良结局相关的特定病毒包括流感病毒、RSV、CMV 和 HSV。同一住院期间同时发生病毒和细菌感染的患者死亡风险最高(RR 6.58,95%CI 5.47-7.91);多器官衰竭(RR 8.25,95%CI 7.50-9.07);和感染性休克(RR 271.2,95%CI 188.0-391.3)。病毒感染可能在 ICU 患者的结局中发挥重要但尚未被认识到的作用。它们可能作为生物标志物,或者通过与同时发生的细菌感染相互作用,在某些不良并发症的发展中发挥积极作用。