Wolfson Institute of Preventive Medicine, Barts and the London School of Medicine and Dentistry, Queen Mary University of London, London, United Kingdom.
PLoS One. 2011 May 4;6(5):e18742. doi: 10.1371/journal.pone.0018742.
Risk factors such as blood pressure and serum cholesterol are used, with age, in screening for future cardiovascular disease (CVD) events. The value of using these risk factors with age compared with using age alone is not known. We compared screening for future CVD events using age alone with screening using age and multiple risk factors based on regular Framingham risk assessments.
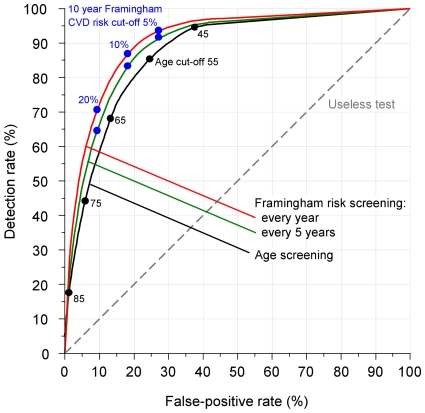
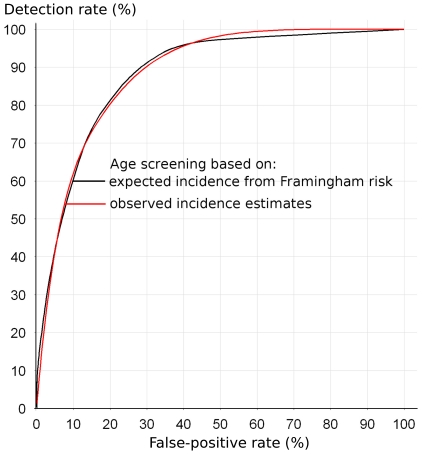
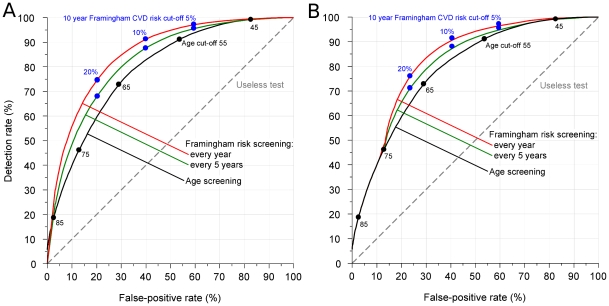
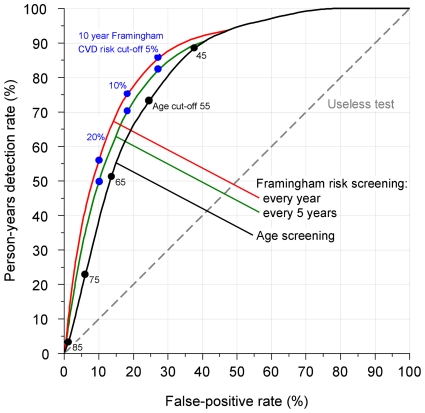
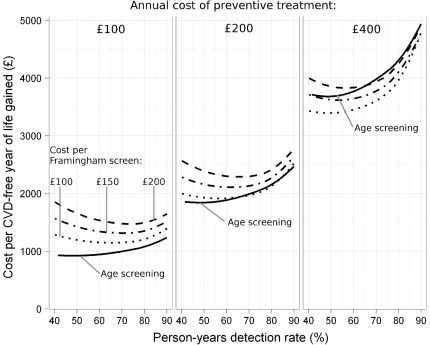
Ten-year CVD risk was estimated using Framingham risk equations in a hypothetical sample population of 500,000 people aged 0-89 years. Risk estimates were used to identify individuals who did and did not have a CVD event over a ten-year period. For screening using age alone (age screening) and screening using multiple risk factors and age (Framingham screening) we estimated the (i) detection rate (sensitivity); (ii) false-positive rate; (iii) proportion of CVD-free years of life lost in affected individuals with positive results (person-years detection rate); and (iv) cost per CVD-free life year gained from preventive treatment.
Age screening using a cut-off of 55 years detected 86% of all first CVD events arising in the population every year and 72% of CVD-free years of life lost for a 24% false-positive rate; for five yearly Framingham screening the false-positive rate was 21% for the same 86% detection rate. The estimated cost per CVD-free year of life gained was £2,000 for age screening and £2,200 for Framingham screening if a Framingham screen costs £150 and the annual cost of preventive treatment is £200.
Age screening for future CVD events is simpler than Framingham screening with a similar screening performance and cost-effectiveness. It avoids blood tests and medical examinations. The advantages of age screening in the prevention of heart attack and stroke warrant considering its use in preference to multiple risk factor screening.
血压和血清胆固醇等危险因素与年龄一起用于筛查未来的心血管疾病 (CVD) 事件。使用这些危险因素与年龄相比单独使用年龄的价值尚不清楚。我们比较了单独使用年龄与使用基于常规弗雷明汉风险评估的年龄和多种危险因素进行未来 CVD 事件筛查的效果。
在一个 50 万人的假设人群中,使用弗雷明汉风险方程估计 10 年 CVD 风险。使用风险估计来确定在 10 年内患有 CVD 事件和未患有 CVD 事件的个体。对于单独使用年龄进行筛查(年龄筛查)和使用多种危险因素和年龄进行筛查(弗雷明汉筛查),我们估计了以下指标:(i)检测率(敏感性);(ii)假阳性率;(iii)阳性结果的个体中 CVD 无病生命年损失的比例(人年检测率);以及(iv)预防治疗获得的每一个 CVD 无病生命年的成本。
使用 55 岁的截止值进行年龄筛查,每年可检测到人群中所有新发 CVD 事件的 86%,并可检测到 CVD 无病生命年损失的 72%,假阳性率为 24%;对于每 5 年进行一次弗雷明汉筛查,相同的 86%检测率下,假阳性率为 21%。如果弗雷明汉筛查的成本为 150 英镑,预防治疗的年度成本为 200 英镑,则年龄筛查获得的每一个 CVD 无病生命年的估计成本为 2000 英镑,而弗雷明汉筛查的成本为 2200 英镑。
与弗雷明汉筛查相比,未来 CVD 事件的年龄筛查更简单,但筛查效果和成本效益相当。它避免了血液测试和体检。年龄筛查在预防心脏病发作和中风方面的优势使得考虑优先使用该方法进行筛查而不是多种危险因素筛查是合理的。