Gamble Jm, Simpson Scot H, Brown Lauren C, Johnson Jeffrey A
Open Med. 2008;2(2):e26-38. Epub 2008 Apr 26.
Although evidence-based guidelines for the treatment of type 2 diabetes mellitus provide clear recommendations for initial therapy, evidence on an optimal treatment strategy after secondary failure is unclear.
To compare the efficacy of add-on therapy using basal insulin versus an additional oral antidiabetic agent in patients with type 2 diabetes and secondary failure.
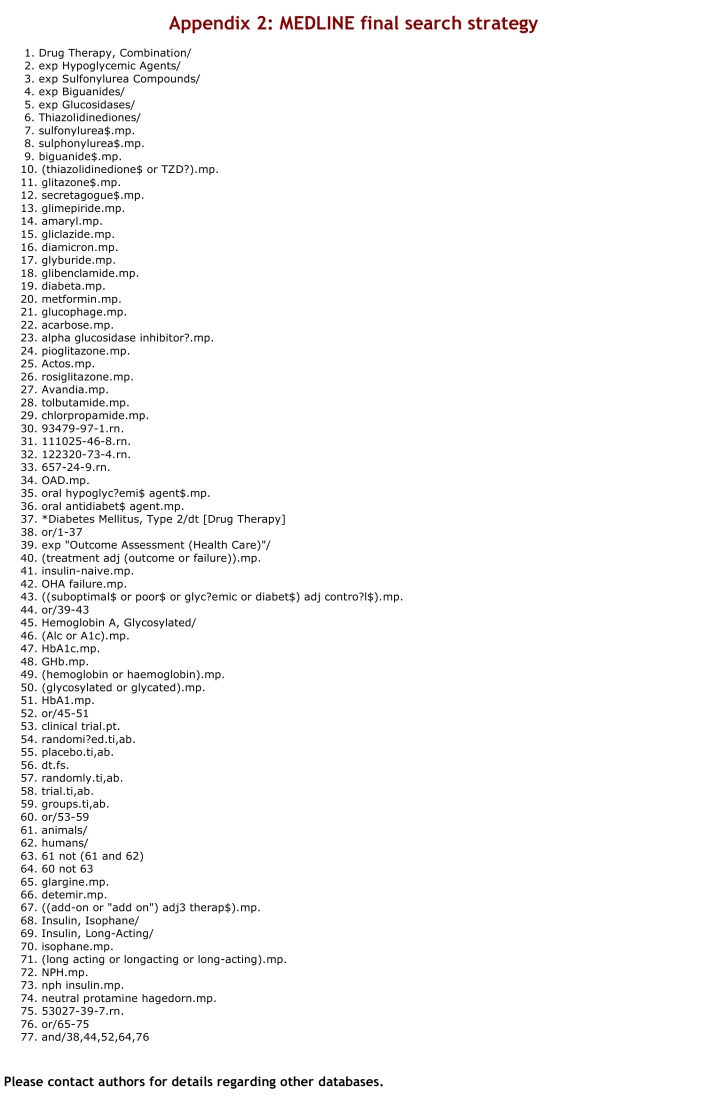
We searched the following electronic databases from inception until June 2007: MEDLINE; EMBASE; Cochrane Central Register of Controlled Trials; Web of Science; Scopus; CINAHL; International Pharmaceutical Abstracts; Academic OneFile; PASCAL; Global Health Database; LILACS; HealthSTAR; PubMed. Reference lists of potentially relevant articles and clinical trial databases were searched, pharmaceutical manufacturers were contacted, and grey literature sources were sought.
Randomized controlled trials (RCTs) involving subjects with type 2 diabetes with secondary failure who were randomly assigned to receive additional basal insulin therapy (insulin glargine, detemir, or NPH [neutral protamine Hagedorn]) versus another oral antidiabetic agent from any class.
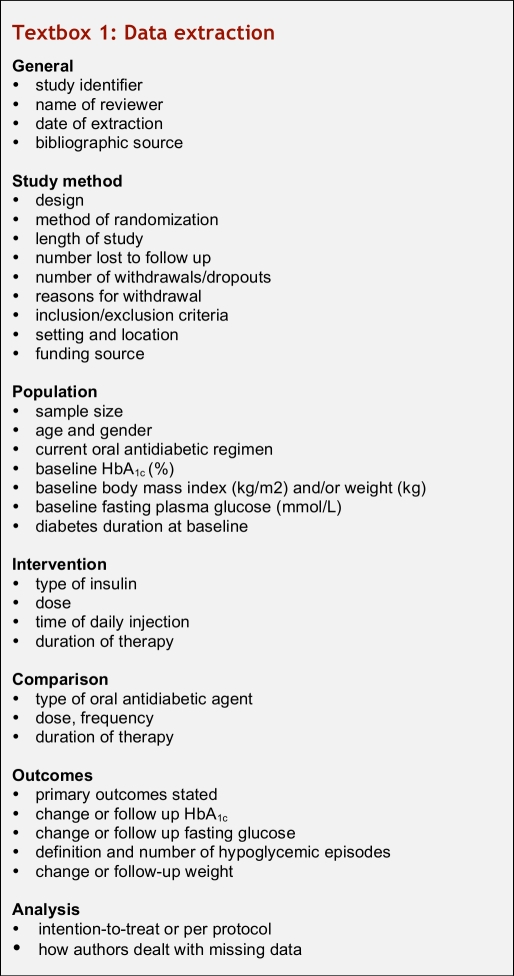
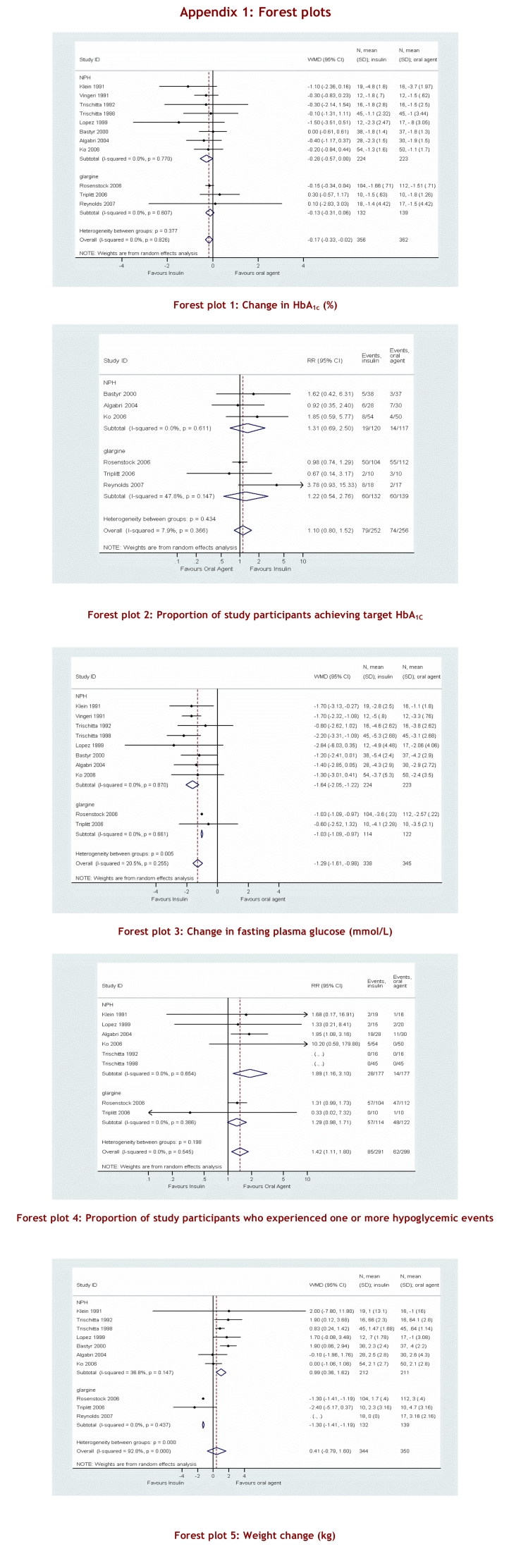
Two reviewers independently screened articles, extracted data and assessed methodological quality. Our primary outcome was glycemic control measured by change in glycosylated hemoglobin (Hb(A1C)) and the proportion of subjects achieving a Hb(A1C) value of ≤ 7%.
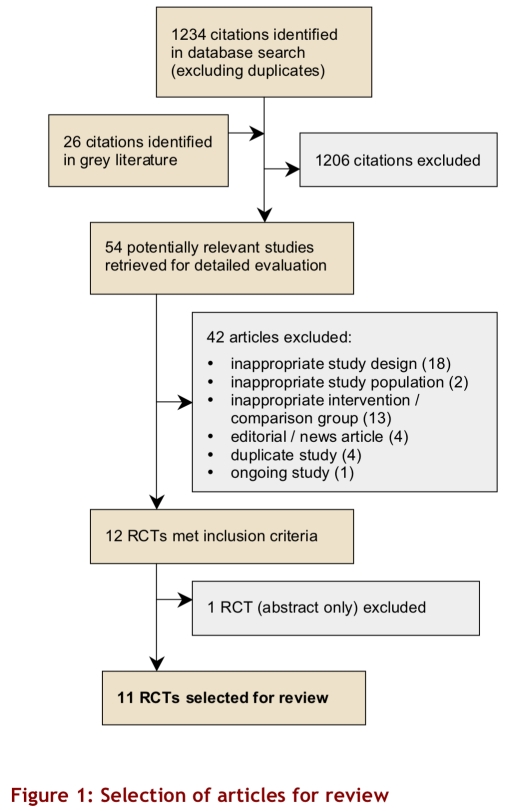
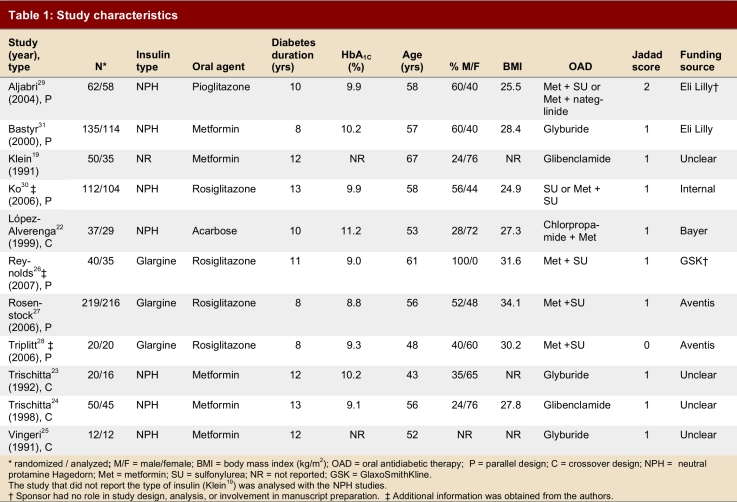
To compare overall efficacy between the 2 treatment strategies, change in Hb(A1C) was pooled across studies using a random-effects model and weighted mean difference (WMD). Eleven RCTs, involving 757 participants with a median age of 56 and a median known duration of diabetes of 11 years, were included in our analysis. Insulin treatment demonstrated a small but statistically significant improvement in Hb(A1C) compared with the use of an additional oral agent as add-on therapy (WMD -0.17; 95% CI [confidence interval] -0.33 to -0.02).
The use of surrogate outcomes and the short duration of the trials makes it impossible to gain information on long-term patient-oriented outcomes. The overall quality of the studies was low, primarily in view of inadequate blinding.
Although add-on therapy using injected insulin shows a slight benefit over an additional oral antidiabetic agent, our results indicate that basal insulin therapy and the use of an oral agent as add-on therapy produce comparable results. Non-therapeutic differences must be considered in the choice of treatment strategies. More high-quality studies with adequate safety data using more aggressive insulin titrations are needed.
尽管2型糖尿病治疗的循证指南对初始治疗给出了明确建议,但关于继发失效后的最佳治疗策略的证据尚不清楚。
比较基础胰岛素联合治疗与加用另一种口服抗糖尿病药物在2型糖尿病继发失效患者中的疗效。
我们检索了以下电子数据库,从建库至2007年6月:医学索引数据库;荷兰医学文摘数据库;考克兰对照试验中心注册库;科学引文索引;Scopus数据库;护理学与健康领域数据库;国际药学文摘数据库;学术大全数据库;帕斯卡数据库;全球健康数据库;拉丁美洲及加勒比地区卫生科学数据库;健康之星数据库;医学期刊数据库。检索了潜在相关文章的参考文献列表和临床试验数据库,联系了制药厂商,并查找了灰色文献来源。
随机对照试验,纳入2型糖尿病继发失效患者,这些患者被随机分配接受额外的基础胰岛素治疗(甘精胰岛素、地特胰岛素或中性鱼精蛋白锌胰岛素)或任何一类其他口服抗糖尿病药物。
两名评价者独立筛选文章、提取数据并评估方法学质量。我们的主要结局是通过糖化血红蛋白(Hb(A1C))变化衡量的血糖控制情况以及达到Hb(A1C)值≤7%的受试者比例。
为比较两种治疗策略的总体疗效,使用随机效应模型和加权均数差(WMD)对各研究中的Hb(A1C)变化进行汇总分析。我们的分析纳入了11项随机对照试验,涉及757名参与者,中位年龄为56岁,已知糖尿病病程中位数为11年。与加用另一种口服药物作为联合治疗相比,胰岛素治疗在Hb(A1C)方面显示出虽小但有统计学意义的改善(WMD -0.17;95%置信区间[CI] -0.33至-0.02)。
使用替代结局以及试验持续时间较短使得无法获得以患者为导向的长期结局信息。研究的总体质量较低,主要是因为盲法不足。
尽管注射胰岛素联合治疗比加用另一种口服抗糖尿病药物显示出轻微益处,但我们的结果表明基础胰岛素治疗和加用口服药物作为联合治疗产生的结果相当。在选择治疗策略时必须考虑非治疗性差异。需要更多采用更积极胰岛素滴定法且有充分安全性数据的高质量研究。