Cardiology Division, GRB800, Department of Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA 02114, USA.
BMC Med. 2011 Jun 24;9:78. doi: 10.1186/1741-7015-9-78.
Drug-eluting stents (DES) reduce rates of restenosis compared with bare metal stents (BMS). A number of observational studies have also found lower rates of mortality and non-fatal myocardial infarction with DES compared with BMS, findings not observed in randomized clinical trials. In order to explore reasons for this discrepancy, we compared outcomes after percutaneous coronary intervention (PCI) with DES or BMS by multiple statistical methods.
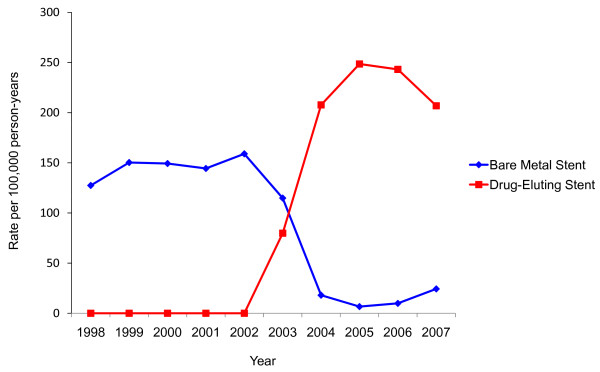
We compared short-term rates of all-cause mortality and myocardial infarction for patients undergoing PCI with DES or BMS using propensity-score adjustment, propensity-score matching, and a stent-era comparison in a large, integrated health system between 1998 and 2007. For the propensity-score adjustment and stent era comparisons, we used multivariable logistic regression to assess the association of stent type with outcomes. We used McNemar's Chi-square test to compare outcomes for propensity-score matching.
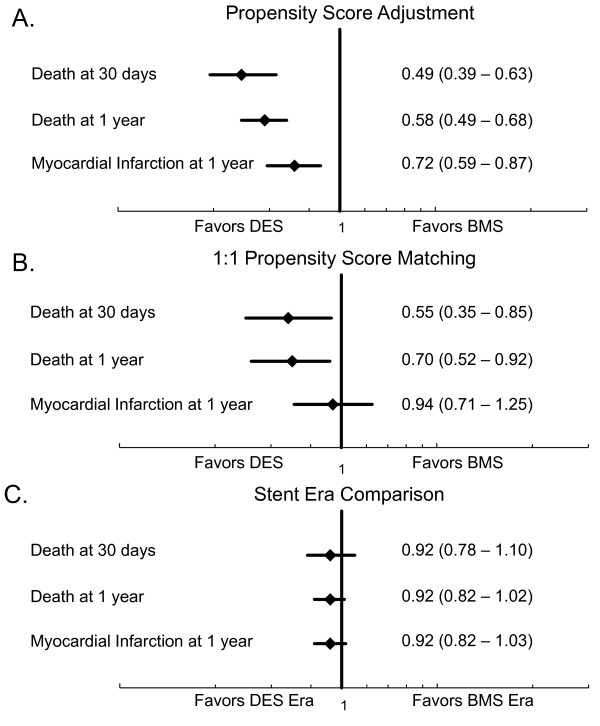
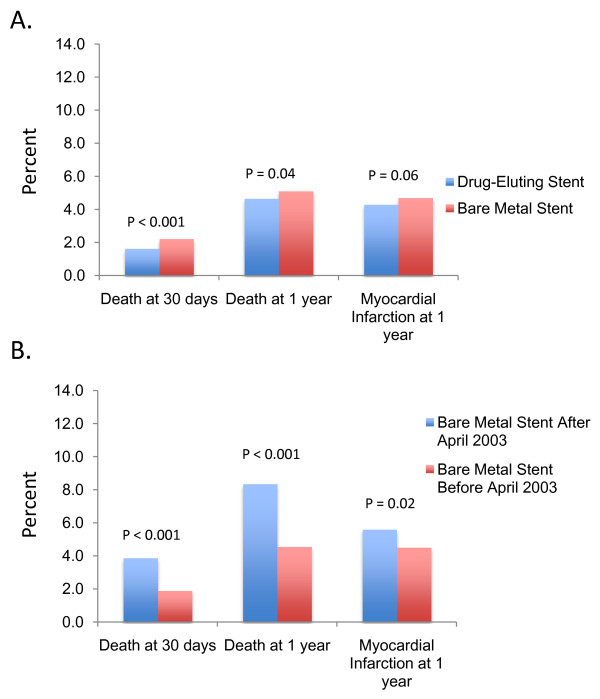
Between 1998 and 2007, 35,438 PCIs with stenting were performed among health plan members (53.9% DES and 46.1% BMS). After propensity-score adjustment, DES was associated with significantly lower rates of death at 30 days (OR 0.49, 95% CI 0.39 - 0.63, P < 0.001) and one year (OR 0.58, 95% CI 0.49 - 0.68, P < 0.001), and a lower rate of myocardial infarction at one year (OR 0.72, 95% CI 0.59 - 0.87, P < 0.001). Thirty day and one year mortality were also lower with DES after propensity-score matching. However, a stent era comparison, which eliminates potential confounding by indication, showed no difference in death or myocardial infarction for DES and BMS, similar to results from randomized trials.
Although propensity-score methods suggested a mortality benefit with DES, consistent with prior observational studies, a stent era comparison failed to support this conclusion. Unobserved factors influencing stent selection in observational studies likely account for the observed mortality benefit of DES not seen in randomized clinical trials.
与裸金属支架(BMS)相比,药物洗脱支架(DES)可降低再狭窄率。一些观察性研究还发现,与 BMS 相比,DES 降低了死亡率和非致死性心肌梗死的发生率,但在随机临床试验中并未观察到这种情况。为了探讨这种差异的原因,我们通过多种统计方法比较了经皮冠状动脉介入治疗(PCI)后使用 DES 或 BMS 的结果。
我们使用倾向评分调整、倾向评分匹配和 1998 年至 2007 年期间大型综合医疗系统中的支架时代比较,比较了接受 DES 或 BMS 治疗的 PCI 患者的短期全因死亡率和心肌梗死发生率。对于倾向评分调整和支架时代比较,我们使用多变量逻辑回归评估支架类型与结局的相关性。我们使用 McNemar 的卡方检验比较倾向评分匹配的结果。
1998 年至 2007 年间,在医疗计划成员中进行了 35438 例 PCI 支架置入术(53.9%为 DES,46.1%为 BMS)。经过倾向评分调整后,DES 与 30 天死亡率(OR 0.49,95%CI 0.39 - 0.63,P < 0.001)和 1 年死亡率(OR 0.58,95%CI 0.49 - 0.68,P < 0.001)显著降低相关,1 年心肌梗死发生率也降低(OR 0.72,95%CI 0.59 - 0.87,P < 0.001)。倾向评分匹配后,30 天和 1 年死亡率也较低。然而,支架时代的比较排除了指示性混杂因素,结果显示 DES 和 BMS 之间在死亡或心肌梗死方面没有差异,与随机试验的结果相似。
尽管倾向评分方法表明 DES 具有死亡率优势,与之前的观察性研究一致,但支架时代的比较未能支持这一结论。观察性研究中影响支架选择的未观察到的因素可能导致观察到的 DES 死亡率优势在随机临床试验中没有出现。