Dept. of Cardiology, Rigshospitalet, Copenhagen University Hospital, Denmark.
BMC Cardiovasc Disord. 2011 Jun 27;11:37. doi: 10.1186/1471-2261-11-37.
Renal function is an important predictor of mortality in patients with myocardial infarction (MI), but changes in the impact over time have not been well described.We examined the importance of renal function by estimated GFR (eGFR) and se-creatinine as an independent long-term prognostic factor.
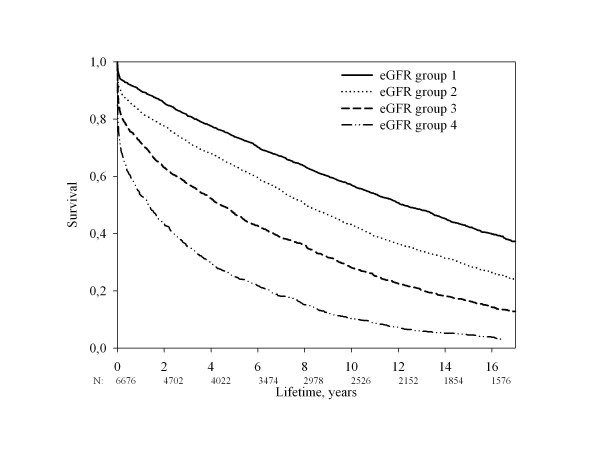
Prospective follow-up of 6653 consecutive MI patients screened for entry in the Trandolapril Cardiac Evaluation (TRACE) study. The patients were analysed by Kaplan-Meier survival analysis, landmark analysis and Cox proportional hazard models. Outcome measure was all-cause mortality.
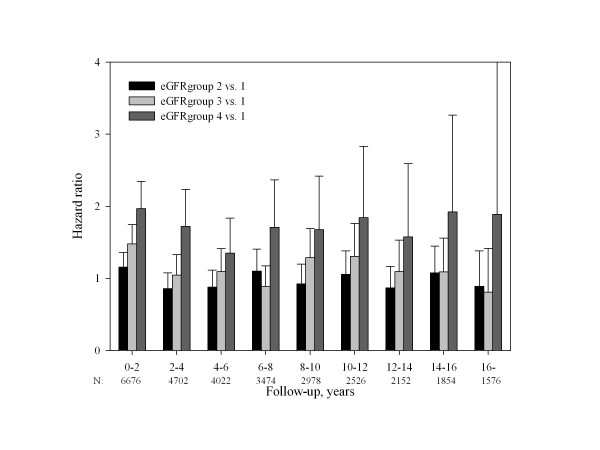
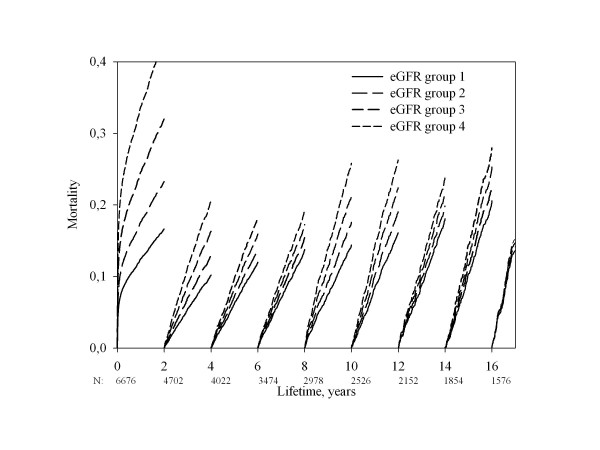
An eGFR below 60 ml per minute per 1.73 m2, consistent with chronic renal disease, was present in 42% of the patients. We divided the patients into 4 groups according to eGFR. Overall, Cox proportional-hazards models showed that eGFR was a significant prognostic factor in the two groups with the lowest eGFR, hazard ratio 1,72 (confidence interval (CI) 1,56-1,91) in the group with the lowest eGFR. Using the eGFR group with normal renal function as reference, we observed an incremental rise in hazard ratio. We divided the follow-up period in 2-year intervals. Landmark analysis showed that eGFR at the time of screening continued to show prognostic effect until 16 years of follow-up. By multivariable Cox regression analysis, the prognostic effect of eGFR persisted for 12 years and of se-creatinine for 10 years. When comparing the lowest group of eGFR with the group with normal eGFR, prognostic significance was present in the entire period of follow-up with a hazard ratio between 1,97 (CI 1,65-2,35) and 1,35 (CI 0,99-1,84) in the 2-year periods.
One estimate of renal function is a strong and independent long-term prognostic factor for 10-12 years following a MI.
肾功能是心肌梗死(MI)患者死亡的重要预测因素,但随着时间的推移,其影响的变化尚未得到很好的描述。我们通过估计肾小球滤过率(eGFR)和血清肌酐来检查肾功能作为独立的长期预后因素的重要性。
对接受特兰洛尔心脏评估(TRACE)研究入选的 6653 例连续 MI 患者进行前瞻性随访。通过 Kaplan-Meier 生存分析、 landmark 分析和 Cox 比例风险模型对患者进行分析。结局指标为全因死亡率。
60 ml/min/1.73 m2 以下的 eGFR,符合慢性肾脏病,存在于 42%的患者中。我们根据 eGFR 将患者分为 4 组。总体而言,Cox 比例风险模型显示 eGFR 在 eGFR 最低的两组中是一个显著的预后因素,eGFR 最低组的危险比为 1.72(置信区间(CI)为 1.56-1.91)。以肾功能正常的 eGFR 组为参考,我们观察到危险比逐渐升高。我们将随访期分为 2 年间隔。landmark 分析显示,筛选时的 eGFR 一直到 16 年的随访仍显示出预后效果。通过多变量 Cox 回归分析,eGFR 的预后效应持续 12 年,血清肌酐的预后效应持续 10 年。当将 eGFR 的最低组与 eGFR 正常组进行比较时,在整个随访期间均存在预后意义,危险比在 1.97(CI 1.65-2.35)和 1.35(CI 0.99-1.84)之间。
MI 后 10-12 年,肾功能的一个估计值是一个强有力的独立长期预后因素。