CMR Unit, Royal Brompton & Harefield NHS Foundation Trust, Sydney Street, London SW3 6NP, UK.
J Cardiovasc Magn Reson. 2011 Jul 6;13(1):34. doi: 10.1186/1532-429X-13-34.
Thalassaemia major (TM) patients need regular blood transfusions that lead to accumulation of iron and death from heart failure. Deferiprone has been reported to be superior to deferoxamine for the removal of cardiac iron and improvement in left ventricular (LV) function but little is known of their relative effects on the right ventricle (RV), which is being increasingly recognised as an important prognostic factor in cardiomyopathy. Therefore data from a prospective randomised controlled trial (RCT) comparing these chelators was retrospectively analysed to assess the RV responses to these drugs.
In the RCT, 61 TM patients were randomised to receive either deferiprone or deferoxamine monotherapy, and CMR scans for T2* and cardiac function were obtained. Data were re-analysed for RV volumes and function at baseline, and after 6 and 12 months of treatment.
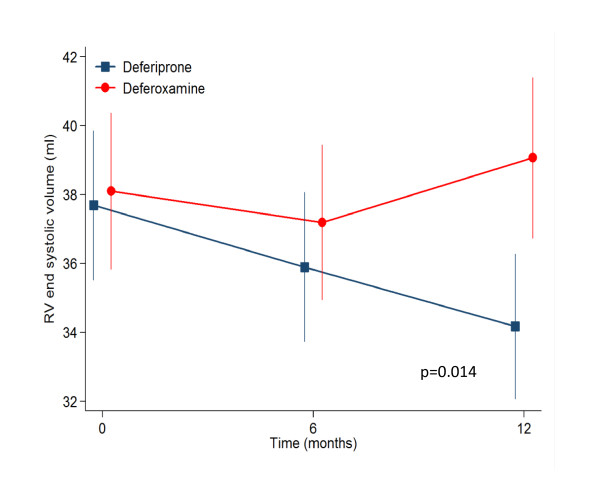
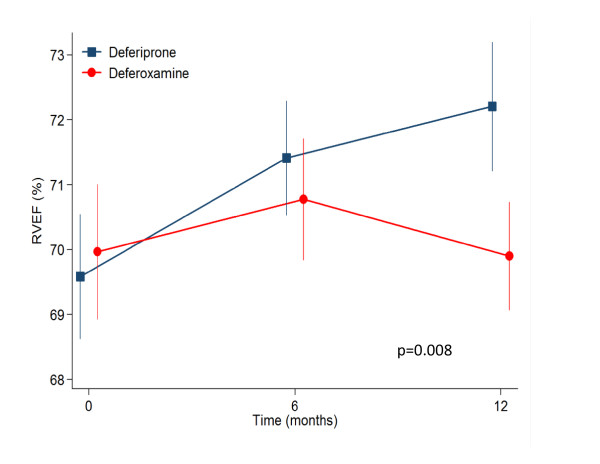
From baseline to 12 months, deferiprone reduced RV end systolic volume (ESV) from 37.7 to 34.2 mL (p=0.008), whilst RV ejection fraction (EF) increased from 69.6 to 72.2% (p=0.001). This was associated with a 27% increase in T2* (p<0.001) and 3.1% increase in LVEF (p<0.001). By contrast, deferoxamine showed no change in RVESV (38.1 to 39.1 mL, p=0.38), or RVEF (70.0 to 69.9%, p=0.93) whereas the T2* increased by 13% (p<0.001), but with no change in LVEF (0.32%; p=0.66). Analysis of between drugs treatment effects, showed significant improvements favouring deferiprone with a mean effect on RVESV of -1.82 mL (p=0.014) and 1.16% for RVEF (p=0.009). Using regression analysis the improvement in RVEF at 12 months was shown to be greater in patients with lower baseline EF values (p<0.001), with a significant difference in RVEF of 3.5% favouring deferiprone over deferoxamine (p=0.012).
In this retrospective analysis of a prospective RCT, deferiprone monotherapy was superior to deferoxamine for improvement in RVEF and end-systolic volume. This improvement in the RV volumes and function may contribute to the improved cardiac outcomes seen with deferiprone.
重型地中海贫血(TM)患者需要定期输血,这会导致铁的积累和心力衰竭死亡。据报道,去铁酮在去除心脏铁和改善左心室(LV)功能方面优于去铁胺,但对于右心室(RV)的相对影响知之甚少,而 RV 作为心肌病的一个重要预后因素,其重要性正日益受到关注。因此,回顾性分析了一项比较这两种螯合剂的前瞻性随机对照试验(RCT)的数据,以评估这些药物对 RV 的影响。
在 RCT 中,61 名 TM 患者被随机分配接受去铁酮或去铁胺单药治疗,并获得 T2*和心脏功能的心脏磁共振(CMR)扫描。在基线、治疗 6 个月和 12 个月时,对 RV 容积和功能进行重新分析。
从基线到 12 个月,去铁酮使 RV 收缩末期容积(ESV)从 37.7 毫升减少到 34.2 毫升(p=0.008),而 RV 射血分数(EF)从 69.6%增加到 72.2%(p=0.001)。这与 T2增加 27%(p<0.001)和 LVEF 增加 3.1%(p<0.001)有关。相比之下,去铁胺对 RVESV(38.1 至 39.1 毫升,p=0.38)或 RVEF(70.0 至 69.9%,p=0.93)均无变化,而 T2增加 13%(p<0.001),但 LVEF 无变化(0.32%;p=0.66)。药物治疗效果的分析表明,去铁酮具有明显的优势,RVESV 平均降低 1.82 毫升(p=0.014),RVEF 增加 1.16%(p=0.009)。回归分析显示,在基线 EF 值较低的患者中,RVEF 的改善更大(p<0.001),去铁酮比去铁胺在 RVEF 方面的优势为 3.5%(p=0.012)。
在这项前瞻性 RCT 的回顾性分析中,去铁酮单药治疗在改善 RVEF 和收缩末期容积方面优于去铁胺。RV 容积和功能的这种改善可能有助于改善去铁酮治疗的心脏结局。