Children's Hospital Boston and Harvard Medical School, Boston, MA 02115, USA.
Am Heart J. 2011 Jul;162(1):125-30. doi: 10.1016/j.ahj.2011.03.021.
The practice of coiling aortopulmonary collaterals (APCs) before Fontan completion is controversial, and published data are limited. We sought to compare outcomes in subjects with and without pre-Fontan coil embolization of APCs using the Pediatric Heart Network Fontan Cross-Sectional Study database which enrolled survivors of prior Fontan palliation.
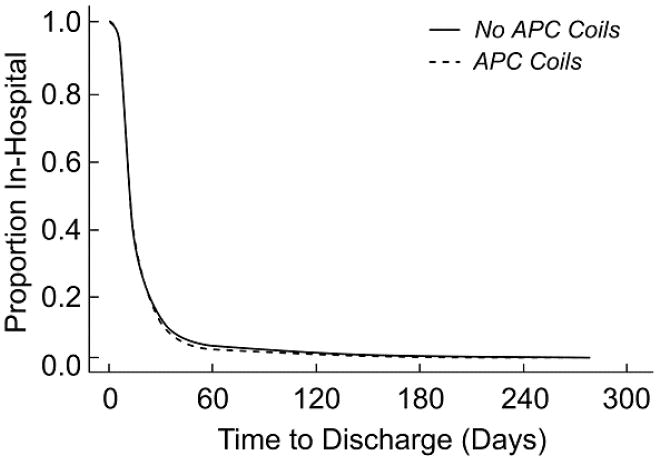
We compared hospital length of stay after Fontan in 80 subjects who underwent APC coiling with 459 subjects who did not. Secondary outcomes included post-Fontan complications and assessment of health status and ventricular performance at cross-sectional evaluation (mean 8.6 ± 3.4 years after Fontan).
Centers varied markedly in frequency of pre-Fontan APC coiling (range 0%-30% of subjects, P < .001). The coil group was older at Fontan (P = .004) and more likely to have single right ventricular morphology (P = .054) and pre-Fontan atrioventricular valve regurgitation (P = .03). The coil group underwent Fontan surgery more recently (P < .001), was more likely to have a prior superior cavopulmonary anastomosis (P < .001), and more likely to undergo extracardiac Fontan connection (P < .001) and surgical fenestration (P < .001). In multivariable analyses, APC coiling was not associated with length of stay (hazard ratio for remaining in-hospital 0.91, 95% CI 0.70-1.18, P = .48) or postoperative complications, except more post-Fontan catheter interventions (hazard ratio 1.74, 95% CI 1.04-2.91, P = .03), primarily additional APC coils. The groups had similar outcomes at cross-sectional evaluation.
Management of APCs before Fontan shows marked practice variation. We did not find an association between pre-Fontan coiling of APCs and shorter postoperative hospital stay or with better late outcomes. Prospective studies of this practice are needed.
在完成 Fontan 手术之前对主肺动脉侧支(APCs)进行线圈栓塞的做法存在争议,并且已发表的数据有限。我们使用小儿心脏网络 Fontan 横截面研究数据库,该数据库招募了先前接受过 Fontan 姑息治疗的幸存者,旨在比较接受和不接受 APC 线圈栓塞的患者在 Fontan 手术后的结局。
我们比较了在 80 例接受 APC 线圈栓塞的患者和 459 例未接受线圈栓塞的患者在 Fontan 手术后的住院时间。次要结局包括 Fontan 后并发症,以及在横截面评估时评估健康状况和心室功能(Fontan 后平均 8.6 ± 3.4 年)。
各中心在 Fontan 前 APC 线圈栓塞的频率上差异显著(范围为 0%-30%的患者,P <.001)。线圈组在 Fontan 时年龄较大(P =.004),更有可能具有单右心室形态(P =.054)和 Fontan 前房室瓣反流(P =.03)。线圈组 Fontan 手术时间较晚(P <.001),更有可能有先前的上腔静脉-肺动脉吻合术(P <.001),更有可能进行心外 Fontan 连接(P <.001)和外科开窗术(P <.001)。多变量分析显示,APC 线圈栓塞与住院时间无关(残留住院时间的风险比为 0.91,95%CI 为 0.70-1.18,P =.48)或术后并发症,除了更多的 Fontan 后导管介入(风险比为 1.74,95%CI 为 1.04-2.91,P =.03),主要是额外的 APC 线圈。两组在横截面评估时的结果相似。
Fontan 前 APC 管理的做法存在明显的差异。我们没有发现 APC 线圈栓塞与术后住院时间缩短或晚期结局改善之间存在关联。需要对此做法进行前瞻性研究。