Kuldeep Cm, Singhal Himanshu, Khare Ashok Kumar, Mittal Asit, Gupta Lalit K, Garg Anubhav
Department of Dermatology, Venereology and Leprosy, RNT Medical College, Udaipur, Rajasthan, India.
Int J Trichology. 2011 Jan;3(1):20-4. doi: 10.4103/0974-7753.82123.
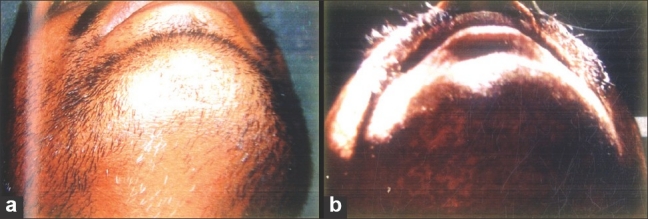
Alopecia areata (AA) is a common, non-scarring, patchy loss of hair at scalp and elsewhere. Its pathogenesis is uncertain; however, auto-immunity has been exemplified in various studies. Familial incidence of AA is 10-42%, but in monozygotic twins is 50%. Local steroids (topical / intra-lesional) are very effective in treatment of localized AA.
To compare hair regrowth and side effects of topical betamethasone valerate foam, intralesional triamcinolone acetonide and tacrolimus ointment in management of localized AA.
105 patients of localized AA were initially registered but 27 were drop out. So, 78 patients allocated at random in group A (28), B (25) and C (25) were prescribed topical betamethasone valerate foam (0.1%) twice daily, intralesional triamcinolone acetonide (10mg/ml) every 3 weeks and tacrolimus ointment (0.1%) twice daily, respectively, for 12 weeks. They were followed for next12 weeks. Hair re-growth was calculated using "HRG Scale"; scale I- (0-25%), S II-(26-50%), S III - (51-75%) and S IV- (75-100%).
Hair re-growth started by 3 weeks in group B (Scale I: P<0.03), turned satisfactory at 6 weeks in group A and B (Scale I: P<0.005, Scale IV: P<0.001)), good at 9 weeks (Scale I: P<0.0005, Scale IV: P<0.00015), and better by 12 weeks of treatment (Scale I: P<0.000021, Scale IV: P<0.000009) in both A and B groups. At the end of 12 weeks follow-up hair re-growth (>75%, HRG IV) was the best in group B (15 of 25, 60%), followed by A (15 of 28, 53.6%) and lastly group-C (Nil of 25, 0%) patients. Few patients reported mild pain and atrophy at injection sites, pruritus and burning with betamethasone valerate foam and tacrolimus.
Intralesional triamcinolone acetonide is the best, betamethasone valerate foam is better than tacrolimus in management of localized AA.
斑秃(AA)是一种常见的、非瘢痕性的头皮及其他部位的斑片状脱发。其发病机制尚不确定;然而,自身免疫在各种研究中已有例证。AA的家族发病率为10 - 42%,但在同卵双胞胎中为50%。局部用类固醇(外用/皮损内注射)对局限性AA的治疗非常有效。
比较外用戊酸倍他米松泡沫、皮损内注射曲安奈德和他克莫司软膏治疗局限性AA时的毛发生长情况及副作用。
105例局限性AA患者最初登记入组,但27例退出。因此,随机分配到A组(28例)、B组(25例)和C组(25例)的78例患者,分别被处方外用0.1%戊酸倍他米松泡沫,每日两次;皮损内注射10mg/ml曲安奈德,每3周一次;外用0.1%他克莫司软膏,每日两次,治疗12周。接下来对他们进行12周的随访。使用“HRG量表”计算毛发生长情况;量表I -(0 - 25%),II级 -(26 - 50%),III级 -(51 - 75%)和IV级 -(75 - 100%)。
B组在3周时开始有毛发生长(I级:P<0.03),A组和B组在6周时毛发生长情况令人满意(I级:P<0.005,IV级:P<0.001),在9周时良好(I级:P<0.0005,IV级:P<0.00015),在治疗12周时更好(I级:P<0.000021,IV级:P<0.000009)。在12周随访结束时,毛发生长情况(>75%,HRG IV级)在B组最佳(25例中的15例,60%),其次是A组(28例中的15例,53.6%),最后是C组(25例中的0例,0%)。少数患者报告注射部位有轻度疼痛和萎缩,使用戊酸倍他米松泡沫和他克莫司时有瘙痒和烧灼感。
在局限性AA的治疗中,皮损内注射曲安奈德效果最佳,戊酸倍他米松泡沫优于他克莫司。