Department of Pediatrics, The Catholic University of Korea College of Medicine, Seoul, Korea.
Yonsei Med J. 2011 Sep;52(5):779-86. doi: 10.3349/ymj.2011.52.5.779.
In this study, we analyzed a cohort of children with chronic graft-versus-host disease (GvHD) according to the NIH consensus classification (NCC) in order to observe whether global assessment at diagnosis correlates with GvHD-specific endpoints. We then studied the clinical course of these patients, specifically with regards to episodes of GvHD exacerbation requiring treatment escalation.
Recipients of either allogeneic bone marrow transplantation (BMT) or peripheral blood stem cell transplantation (PBSCT) from January 2006 to August 2008 at the Department of Pediatrics, The Catholic University of Korea were evaluated for chronic GvHD, which was diagnosed according to the NCC. The course of chronic GvHD in these patients was then followed.
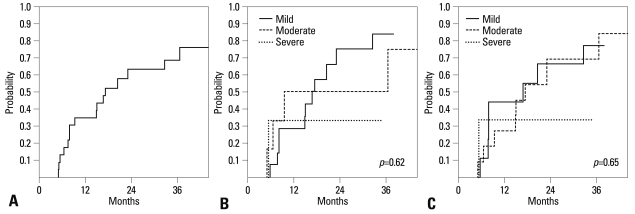
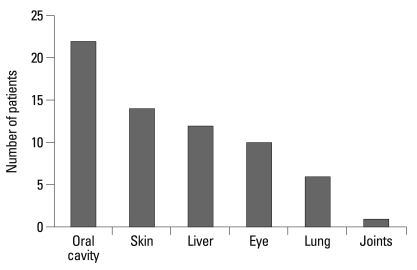
Of 59 evaluable patients, 23 developed chronic GvHD for a cumulative incidence of 39.3%. Upon multivariate analysis, previous acute GvHD (≥grade II) had a significant impact on chronic GvHD incidence. With a median duration of systemic treatment for chronic GvHD of 501 days, no significant relationship was found between initial global severity of chronic GvHD and either duration of immunosuppressive treatment or final clinical response to treatment. Fifteen patients (65%) experienced at least one episode of chronic GvHD exacerbation during the period of follow-up, with a median of four exacerbations in the subgroup of patients who experienced such events. Lung GvHD resulted in the highest number of exacerbations per diagnosed patient, followed by oral GvHD.
Analysis of this small cohort indicates that global assessment as proposed by the NCC may have limited correlations with GvHD-specific endpoints, possibly due to the favorable response of children to treatment.
本研究根据 NIH 共识分类(NCC)分析了一组患有慢性移植物抗宿主病(GvHD)的儿童队列,以观察诊断时的总体评估是否与 GvHD 特异性终点相关。然后,我们研究了这些患者的临床病程,特别是需要治疗升级的 GvHD 加重发作的情况。
2006 年 1 月至 2008 年 8 月,韩国天主教大学儿科的所有接受异基因骨髓移植(BMT)或外周血干细胞移植(PBSCT)的患者均接受了慢性 GvHD 的评估,诊断标准为 NCC。然后对这些患者的慢性 GvHD 病程进行了随访。
在 59 例可评估的患者中,23 例发生慢性 GvHD,累积发生率为 39.3%。多变量分析显示,既往急性 GvHD(≥Ⅱ级)对慢性 GvHD 发生率有显著影响。慢性 GvHD 的系统性治疗中位持续时间为 501 天,但初始慢性 GvHD 的总体严重程度与免疫抑制治疗的持续时间或最终治疗的临床反应之间未发现显著关系。在随访期间,15 例(65%)患者至少经历了一次慢性 GvHD 加重发作,其中经历过此类事件的患者亚组的中位发作次数为 4 次。肺部 GvHD 导致每例确诊患者的加重发作次数最多,其次是口腔 GvHD。
对这一小队列的分析表明,NCC 提出的总体评估可能与 GvHD 特异性终点相关性有限,这可能是由于儿童对治疗的良好反应。