Center for Clinical Heart Research, Oslo University Hospital, Ullevål, Oslo, Norway.
BMC Endocr Disord. 2011 Jul 29;11:14. doi: 10.1186/1472-6823-11-14.
Patients with acute myocardial infarction and newly detected abnormal glucose regulation have been shown to have a less favourable prognosis compared to patients with normal glucose regulation. The importance and timing of oral glucose tolerance testing (OGTT) in patients with acute myocardial infarction without known diabetes is uncertain. The aim of the present study was to evaluate the impact of abnormal glucose regulation classified by an OGTT in-hospital and at three-month follow-up on clinical outcome in patients with acute ST elevation myocardial infarction (STEMI) without known diabetes.
Patients (n = 224, age 58 years) with a primary percutanous coronary intervention (PCI) treated STEMI were followed for clinical events (all-cause mortality, non-fatal myocardial re-infarction, recurrent ischemia causing hospital admission, and stroke). The patients were classified by a standardised 75 g OGTT at two time points, first, at a median time of 16.5 hours after hospital admission, then at three-month follow-up. Based on the OGTT results, the patients were categorised according to the WHO criteria and the term abnormal glucose regulation was defined as the sum of impaired fasting glucose, impaired glucose tolerance and type 2-diabetes.
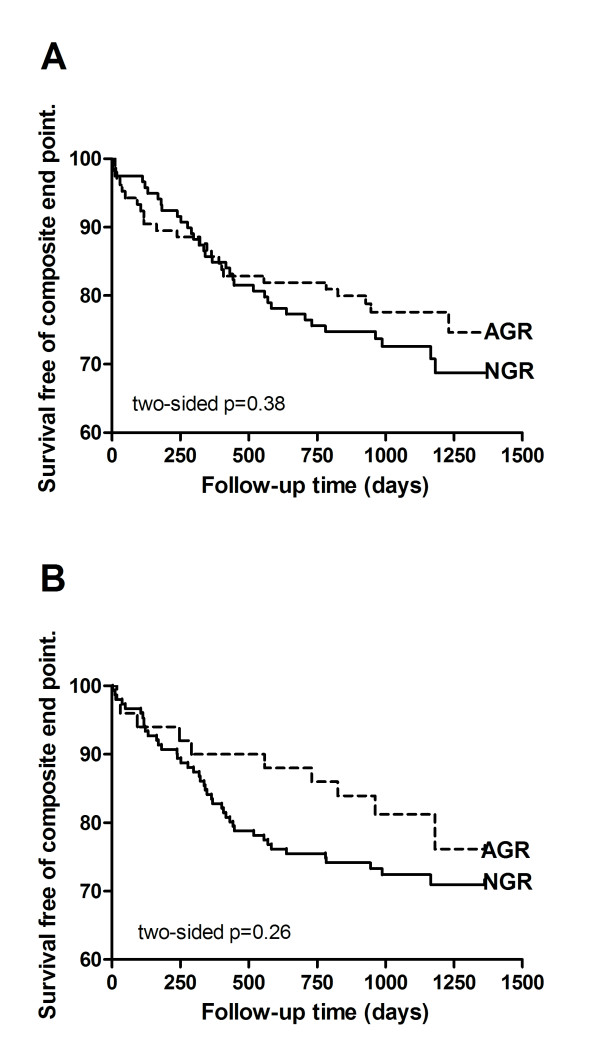
The number of patients diagnosed with abnormal glucose regulation in-hospital and at three-month was 105 (47%) and 50 (25%), respectively. During the follow up time of (median) 33 (27, 39) months, 58 (25.9%) patients experienced a new clinical event. There were six deaths, 15 non-fatal re-infarction, 33 recurrent ischemia, and four strokes. Kaplan-Meier analysis of survival free of composite end-points showed similar results in patients with abnormal and normal glucose regulation, both when classified in-hospital (p = 0.4) and re-classified three months later (p = 0.3).
Patients with a primary PCI treated STEMI, without previously known diabetes, appear to have an excellent long-term prognosis, independent of the glucometabolic state classified by an OGTT in-hospital or at three-month follow-up.
The trial is registered at http://www.clinicaltrials.gov, NCT00926133.
与血糖调节正常的患者相比,急性心肌梗死伴新发现的异常血糖调节患者的预后较差。对于无糖尿病病史的急性心肌梗死患者,口服葡萄糖耐量试验(OGTT)的重要性和时机尚不确定。本研究旨在评估入院时和 3 个月随访时 OGTT 异常葡萄糖调节对无糖尿病病史的急性 ST 段抬高型心肌梗死(STEMI)患者临床结局的影响。
对 224 例接受经皮冠状动脉介入治疗(PCI)的原发性 STEMI 患者进行随访,以评估临床事件(全因死亡率、非致死性心肌再梗死、复发性缺血导致住院和卒中)的发生情况。患者于入院后 16.5 小时的中位数时间内和 3 个月随访时,进行标准 75 g OGTT 检查,并根据 OGTT 结果,按照世界卫生组织(WHO)标准进行分类。异常葡萄糖调节的定义为空腹血糖受损、葡萄糖耐量受损和 2 型糖尿病之和。
入院时和 3 个月时诊断为异常葡萄糖调节的患者分别为 105 例(47%)和 50 例(25%)。在(中位数)33(27,39)个月的随访期间,58 例(25.9%)患者发生新的临床事件。其中 6 例死亡,15 例非致死性再梗死,33 例复发性缺血,4 例卒中等。无复合终点生存的 Kaplan-Meier 分析显示,入院时和 3 个月时,异常葡萄糖调节组和正常葡萄糖调节组的结果相似(入院时:p=0.4;3 个月时:p=0.3)。
对于无糖尿病病史的接受原发性 PCI 治疗的 STEMI 患者,无论入院时还是 3 个月时 OGTT 异常葡萄糖调节的分类如何,患者似乎都具有极好的长期预后。
本试验在 clinicaltrials.gov 注册,NCT00926133。