Department of Infectious Diseases, Institute for Viral Hepatitis, Key Laboratory of Molecular Biology for Infectious Diseases, Ministry of Education, The Second Affiliated Hospital of Chongqing Medical University, China.
Virol J. 2011 Aug 8;8:393. doi: 10.1186/1743-422X-8-393.
Chronic hepatitis B virus (HBV) infection represents a serious global health problem and resistance to lamivudine (LAM) has become a serious clinical challenge. Previous rescue therapy for the treatment of chronic LAM-resistant hepatitis B infected patients included switching to entecavir (ETV) and adding adefovir (ADV) or tenofovir (TFV). At present, switching to ETV is not recommended for rescue therapy for LAM-resistant chronic hepatitis B (CHB). The aim of this report was to determine whether add-on ADV was a superior rescue strategy in the treatment of CHB patients with LAM resistance.
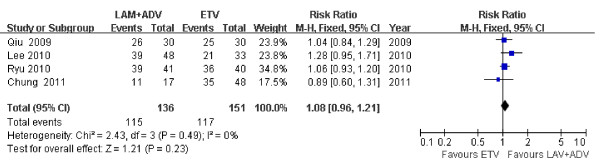
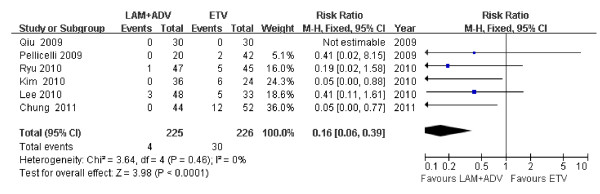
We searched Medline/PubMed, EMBASE, Web of Knowledge, and the Cochrane Library. Relative risks (RRs) of virologic response, virologic breakthrough, normalization of serum alanine aminotransferase (ALT) levels and HBeAg seroconversion rates were studied. Factors predicting virologic response, standardized mean differences (SMD) in HBV DNA levels and safety were reviewed.
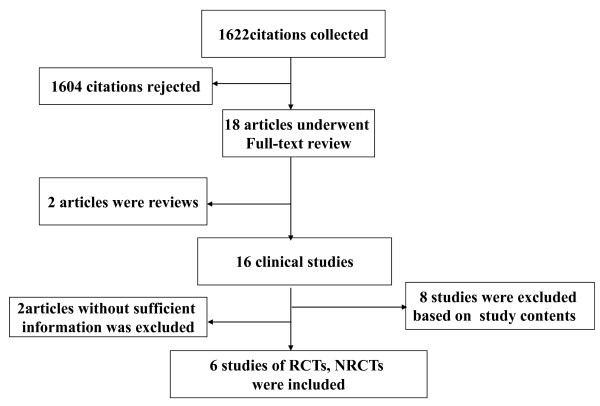
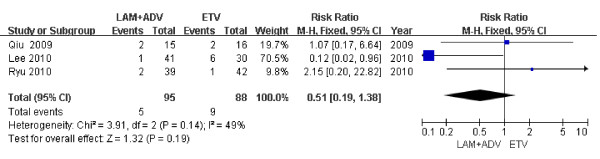
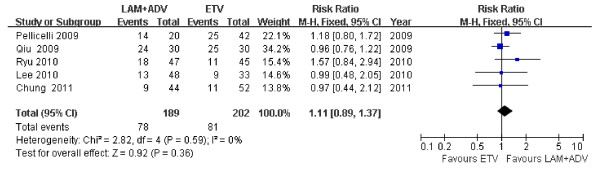
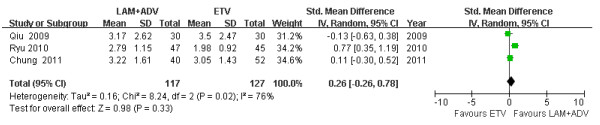
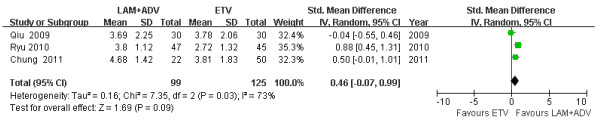
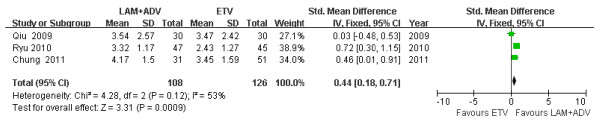
Six eligible trials (451 patients in total) were included in the analysis. The rate of virologic breakthrough in the ETV group was higher than that in the LAM plus ADV group. There were no statistical differences in virologic response, ALT normalization and HBeAg seroconversion in either group 48 weeks post treatment. LAM plus ADV combination therapy produced faster and greater HBV DNA reduction rates 24 weeks post therapy compared to ETV monotherapy. HBV DNA baseline levels and the initial virologic response (IVR) were predictive of the virologic response. Additionally, combination therapy or monotherapy were both well tolerated.
LAM plus ADV combination therapy was more effective and produced longer-lasting effects than switching to ETV monotherapy in treating CHB patients with LAM resistance. However, considering the practical benefits and limitations of ADV, individualized therapy will be needed in patients with prior history of LAM resistant infections.
慢性乙型肝炎病毒(HBV)感染是一个严重的全球健康问题,对拉米夫定(LAM)的耐药性已成为一个严重的临床挑战。先前用于治疗慢性 LAM 耐药性乙型肝炎感染患者的挽救治疗包括转为恩替卡韦(ETV)并加用阿德福韦(ADV)或替诺福韦(TFV)。目前,不建议将转为 ETV 用于 LAM 耐药性慢性乙型肝炎(CHB)的挽救治疗。本报告旨在确定在治疗 LAM 耐药性 CHB 患者时,加用 ADV 是否是一种更好的挽救策略。
我们检索了 Medline/PubMed、EMBASE、Web of Knowledge 和 Cochrane 图书馆。研究了病毒学应答、病毒学突破、血清丙氨酸氨基转移酶(ALT)水平正常化和 HBeAg 血清学转换率的相对风险(RR)。还回顾了预测病毒学应答的因素、HBV DNA 水平的标准化均数差(SMD)和安全性。
纳入了 6 项符合条件的试验(共 451 例患者)进行分析。ETV 组的病毒学突破率高于 LAM 加 ADV 组。治疗后 48 周,两组在病毒学应答、ALT 正常化和 HBeAg 血清学转换方面均无统计学差异。与 ETV 单药治疗相比,LAM 加 ADV 联合治疗在治疗 LAM 耐药性 CHB 患者时能更快、更持久地降低 HBV DNA 水平。HBV DNA 基线水平和初始病毒学应答(IVR)是病毒学应答的预测因素。此外,联合治疗或单药治疗均具有良好的耐受性。
与转为 ETV 单药治疗相比,LAM 加 ADV 联合治疗在治疗 LAM 耐药性 CHB 患者时更有效,且疗效持续时间更长。然而,考虑到 ADV 的实际效益和局限性,对于有 LAM 耐药感染既往史的患者,需要个体化治疗。