Division of Nuclear Medicine, Washington Hospital Center, Washington, DC 20010-2910, USA.
J Clin Endocrinol Metab. 2011 Oct;96(10):3217-25. doi: 10.1210/jc.2011-0494. Epub 2011 Aug 17.
The optimal management of high-risk patients with differentiated thyroid cancer (DTC) consists of thyroidectomy followed by radioiodine ((131)I) therapy. The prescribed activity of (131)I can be determined using two approaches: 1) empiric prescribed activity of (131)I (E-Rx); and 2) dosimetry-based prescribed activity of (131)I (D-Rx).
The aim of the study was to compare the relative treatment efficacy and side effects of D-Rx vs. E-Rx.
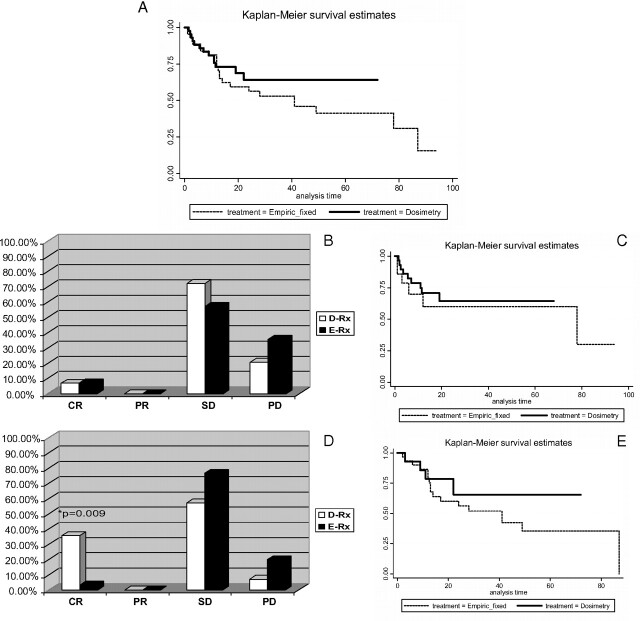
A retrospective analysis was performed of patients with distant metastases and/or locoregionally advanced radioiodine-avid DTC who were treated with either D-Rx or E-Rx. Response to treatment was based on RECIST (Response Evaluation Criteria in Solid Tumors) 1.1 criteria.
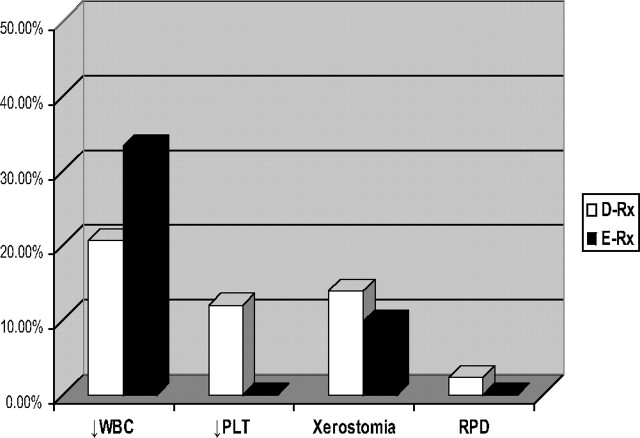
The study group consisted of 87 patients followed for 51 ± 35 months, of whom 43 were treated with D-Rx and 44 with E-Rx. Multivariate analysis, controlling for age, gender, and status of metastases revealed that the D-Rx group tended to be 70% less likely to progress (odds ratio, 0.29; 95% confidence interval, 0.087-1.02; P = 0.052) and more likely to obtain complete response (CR) compared to the E-Rx group (odds ratio, 8.2; 95% confidence interval, 1.2-53.5; P = 0.029). There was an association in the D-Rx group between the observed CR and percentage of maximum tolerable activity given as a first treatment of (131)I (P = 0.030). The advantage of D-Rx was specifically apparent in the locoregionally advanced group because CR was significantly higher in D-Rx vs. E-Rx in this group of patients (35.7 vs. 3.3%; P = 0.009). The rates of partial response, stable disease, and progression-free survival, as well as the frequency of side effects, were not significantly different between the two groups.
Higher efficacy of D-Rx with a similar safety profile compared to E-Rx supports the rationale for employing individually prescribed activity in high-risk patients with DTC.
分化型甲状腺癌(DTC)高危患者的最佳治疗方案包括甲状腺切除术联合放射性碘((131)I)治疗。(131)I 的推荐活度可以通过两种方法确定:1)经验性推荐活度 (E-Rx);2)基于剂量学的推荐活度 (D-Rx)。
本研究旨在比较 D-Rx 与 E-Rx 的相对治疗效果和副作用。
回顾性分析了接受 D-Rx 或 E-Rx 治疗的远处转移和/或局部晚期放射性碘摄取阳性 DTC 患者。根据 RECIST(实体瘤反应评价标准)1.1 标准评价治疗反应。
本研究共纳入 87 例患者,中位随访时间为 51±35 个月,其中 43 例接受 D-Rx 治疗,44 例接受 E-Rx 治疗。多变量分析,控制年龄、性别和转移状态后,发现 D-Rx 组疾病进展的风险比 E-Rx 组低 70%(比值比,0.29;95%置信区间,0.087-1.02;P=0.052),且更容易获得完全缓解(CR)(比值比,8.2;95%置信区间,1.2-53.5;P=0.029)。在 D-Rx 组中,观察到的 CR 与首次 (131)I 治疗给予的最大耐受活度百分比之间存在关联(P=0.030)。D-Rx 的优势在局部晚期组中更为明显,因为在该组患者中,D-Rx 组的 CR 明显高于 E-Rx 组(35.7% vs. 3.3%;P=0.009)。两组间部分缓解、疾病稳定和无进展生存率以及副作用发生率无显著差异。
与 E-Rx 相比,D-Rx 的疗效更高,安全性相似,支持对高危 DTC 患者采用个体化推荐活度的合理性。