1. Breast Cancer Translational Research Laboratory, The University of Texas MD Anderson Cancer Center, Houston, Texas;
J Cancer. 2011;2:435-42. doi: 10.7150/jca.2.435. Epub 2011 Aug 7.
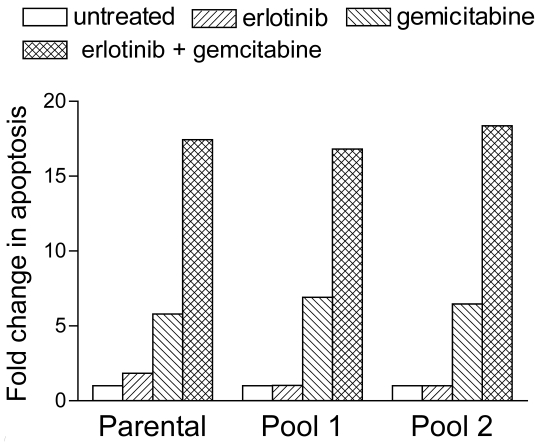
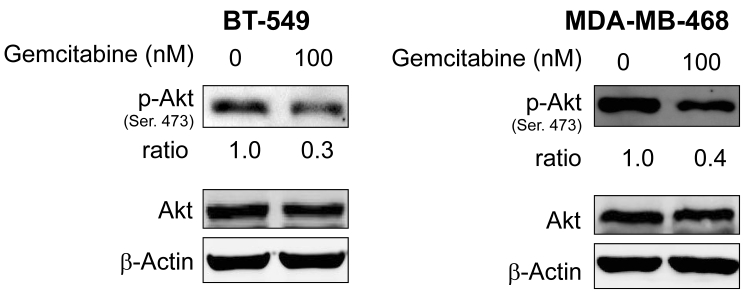
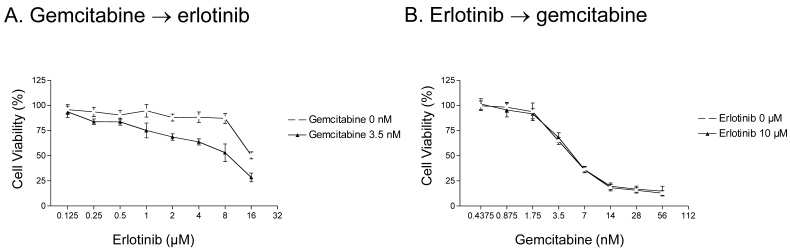
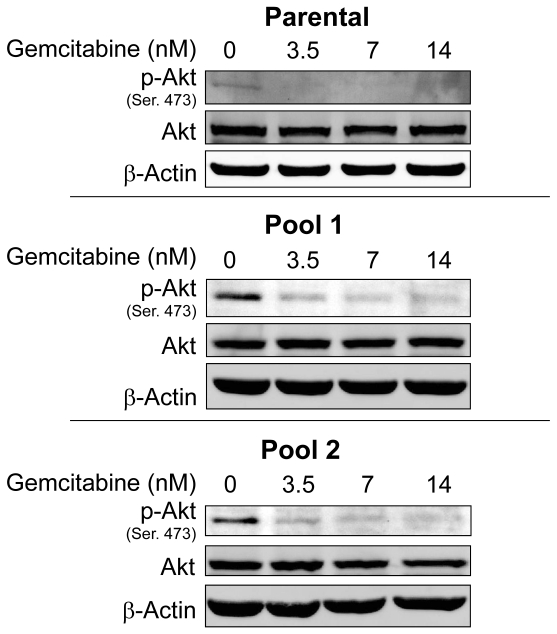
A phase III clinical trial showed gemcitabine chemotherapy combined with epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor erlotinib significantly improved overall survival in patients with advanced pancreatic cancer. Therefore, we studied whether addition of gemcitabine to erlotinib in cancer cells having intrinsic or acquired erlotinib resistance could restore chemosensitization in these cells. We studied the synergistic effect of erlotinib and gemcitabine in EGFR-overexpressing A-431 cells with acquired erlotinib resistance and in intrinsic erlotinib-resistant triple negative breast cancer (TNBC) BT-549, MDA-MB-231 and MDA-MB-468 cell lines. Erlotinib and gemcitabine were synergistic in both parental intrinsically erlotinib-sensitive A-431 cells (combination index = 0.69 at the effective dose [ED(50)]) and in two A-431 cell pools that had acquired erlotinib resistance (combination indices = 0.63 and 0.49 at ED(50)). The synergistic effect of erlotinib and gemcitabine on cancer cells did not require sensitivity to erlotinib provided that erlotinib can inhibit EGFR. The restoration of sensitivity by gemcitabine occurred through downregulation of phosphorylated Akt (p-Akt), which suggests that PI3K-PTEN-Akt activity is important to the synergism between the two agents. In A-431 parental cells, treatment with gemcitabine followed by erlotinib - but not the reverse sequence - was superior to erlotinib alone. The importance of the order of administration maybe due to the downregulation of p-Akt by gemcitabine in a dose- and time-dependent manner in cells with intrinsic or acquired erlotinib resistance. Our data show that gemcitabine increased the cytotoxic effect of erlotinib by downregulating p-Akt in EGFR-overexpressing cells with either intrinsic or acquired erlotinib resistance.
一项 III 期临床试验表明,吉西他滨化疗联合表皮生长因子受体(EGFR)酪氨酸激酶抑制剂厄洛替尼可显著改善晚期胰腺癌患者的总生存期。因此,我们研究了在具有内在或获得性厄洛替尼耐药性的癌细胞中添加吉西他滨是否可以恢复这些细胞的化疗敏感性。我们研究了 EGFR 过表达的 A-431 细胞中获得性厄洛替尼耐药和内在厄洛替尼耐药的三阴性乳腺癌(TNBC)BT-549、MDA-MB-231 和 MDA-MB-468 细胞系中厄洛替尼和吉西他滨的协同作用。厄洛替尼和吉西他滨在亲本内在厄洛替尼敏感的 A-431 细胞(有效剂量[ED(50)]的组合指数为 0.69)和两个获得性厄洛替尼耐药的 A-431 细胞池中均具有协同作用(ED(50)的组合指数为 0.63 和 0.49)。厄洛替尼和吉西他滨对癌细胞的协同作用不要求对厄洛替尼敏感,只要厄洛替尼能抑制 EGFR。吉西他滨通过下调磷酸化 Akt(p-Akt)恢复敏感性,这表明 PI3K-PTEN-Akt 活性对两种药物的协同作用很重要。在 A-431 亲本细胞中,吉西他滨后用厄洛替尼治疗 - 而不是相反的顺序 - 优于单独使用厄洛替尼。给药顺序的重要性可能是由于吉西他滨在内在或获得性厄洛替尼耐药的细胞中以剂量和时间依赖性方式下调 p-Akt。我们的数据表明,吉西他滨通过下调 EGFR 过表达细胞中的 p-Akt,增加了厄洛替尼的细胞毒性作用,无论这些细胞是内在还是获得性耐药。