Division of Neonatal-Perinatal Medicine, Department of Pediatrics, College of Medicine, The Ohio State University, Columbus, OH 43210-1228, USA.
J Perinatol. 2012 Jun;32(6):425-30. doi: 10.1038/jp.2011.114. Epub 2011 Aug 18.
Each year in the US ∼50 000 neonates receive inpatient pharmacotherapy for the treatment of neonatal abstinence syndrome (NAS). The objective of this study is to compare the safety and efficacy of a traditional inpatient only approach with a combined inpatient and outpatient methadone treatment program.
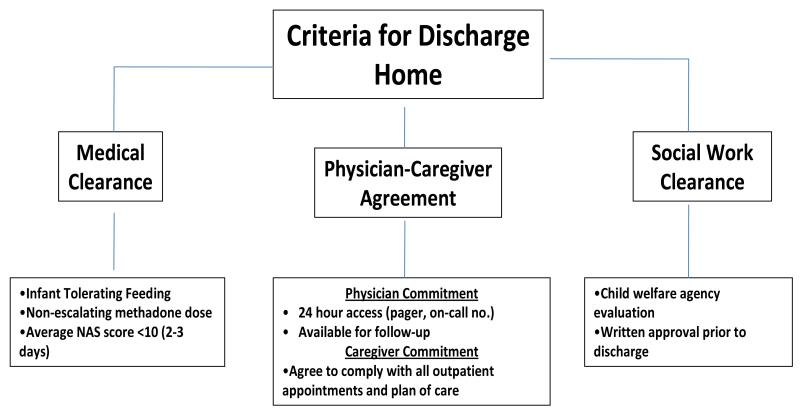
Retrospective review (2007 to 2009). Infants were born to mothers maintained on methadone in an antenatal substance abuse program. All infants received methadone for NAS treatment as inpatient. Methadone weaning for the traditional group (75 patients) was inpatient, whereas the combined group (46 patients) was outpatient.
Infants in the traditional and combined groups were similar in demographics, obstetrical risk factors, birth weight, gestational age (GA) and the incidence of prematurity (34 and 31%). Hospital stay was shorter in the combined than in the traditional group (13 vs 25 days; P<0.01). Although the duration of treatment was longer for infants in the combined group (37 vs 21 days, P<0.01), the cumulative methadone dose was similar (3.6 vs 3.1 mg kg(-1), P=0.42). Follow-up information (at least 3 months) was available for 80% of infants in the traditional and 100% of infants in the combined group. All infants in the combined group were seen ≤72 h from hospital discharge. Breastfeeding was more common among infants in the combined group (24 vs 8% P<0.05). Following discharge there were no differences between the two groups in hospital readmissions for NAS. Prematurity (34 to 36 weeks GA) was the only predictor for hospital readmission for NAS in both groups (P=0.02, OR 5). Average hospital cost for each infant in the combined group was $13 817 less than in the traditional group.
A combined inpatient and outpatient methadone treatment in the management of NAS decreases hospital stay and substantially reduces cost. Additional studies are needed to evaluate the potential long-term benefits of the combined approach on infants and their families.
在美国,每年有大约 50000 名新生儿因治疗新生儿戒断综合征(NAS)而接受住院药物治疗。本研究旨在比较传统的住院治疗方法与住院和门诊美沙酮联合治疗方案的安全性和疗效。
回顾性研究(2007 年至 2009 年)。婴儿的母亲在产前药物滥用计划中接受美沙酮治疗。所有婴儿均接受美沙酮治疗 NAS。传统组(75 例)的美沙酮停药为住院,而联合组(46 例)为门诊。
传统组和联合组的婴儿在人口统计学、产科危险因素、出生体重、胎龄(GA)和早产发生率(34%和 31%)方面相似。联合组的住院时间短于传统组(13 天比 25 天;P<0.01)。尽管联合组婴儿的治疗时间较长(37 天比 21 天,P<0.01),但累积美沙酮剂量相似(3.6 毫克/千克比 3.1 毫克/千克,P=0.42)。传统组有 80%的婴儿和联合组有 100%的婴儿获得了随访信息(至少 3 个月)。联合组所有婴儿均在出院后 72 小时内就诊。联合组婴儿母乳喂养更为常见(24%比 8%,P<0.05)。出院后,两组因 NAS 再次住院的患儿无差异。早产(GA34 至 36 周)是两组患儿因 NAS 再次住院的唯一预测因素(P=0.02,OR 5)。联合组每名婴儿的平均住院费用比传统组低 13817 美元。
NAS 管理中美沙酮的住院和门诊联合治疗可缩短住院时间,显著降低成本。需要进一步研究评估联合治疗对婴儿及其家庭的潜在长期益处。