Liver Transplantation Center, Third Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, China.
PLoS One. 2011;6(9):e25295. doi: 10.1371/journal.pone.0025295. Epub 2011 Sep 26.
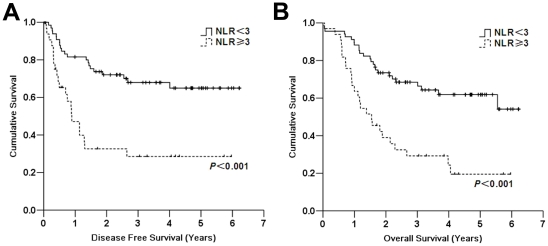
Neutrophil to lymphocyte ratio (NLR) has been proposed to predict prognosis of hepatocellular carcinoma (HCC). However, the cut-off values are empirical. We determined the optimal cut-off value to predict HCC recurrence after liver transplantation (LT) and further established a scoring model based on NLR.
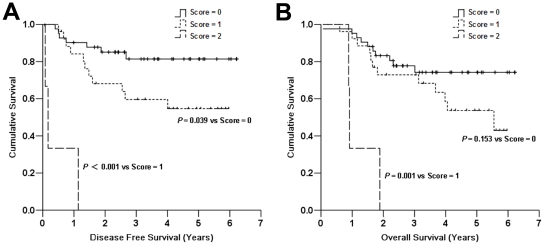
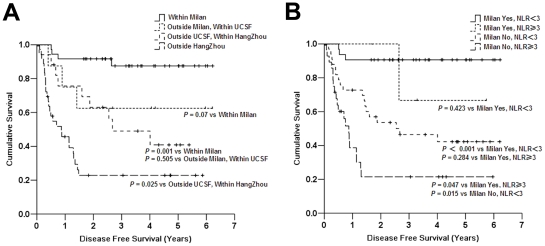
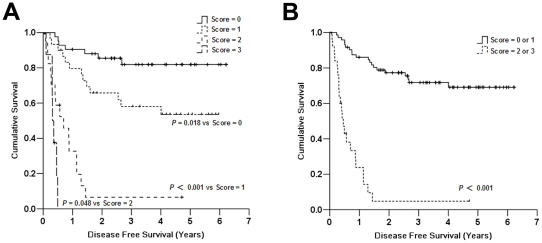
METHODOLOGY/PRINCIPAL FINDINGS: We analyzed the outcome of 101 HBV-associated HCC patients undergoing LT. Preoperative risk factors for tumor recurrence were evaluated by univariate analysis. By using ROC analysis, NLR≥3 was considered elevated. The disease-free survival (DFS) and overall survival (OS) for patients with high NLR was significantly worse than that for patients with normal NLR (the 5-year DFS and OS of 28.5% and 19.5% vs. 64.9% and 61.8%, respectively; P<0.001). Univariate analysis revealed that tumor size >5 cm, tumor number >3, macrovascular invasion, AFP≥400 µg/L, NLR≥3, and HBV-DNA level >5 log10 copies/mL were preoperative predictors of DFS. Cox regression analysis showed macrovascular invasion, tumor number, and high NLR were independent prognostic factors. We then established a preoperative prognostic score based on multivariate analysis. Each factor was given a score of 1. Area under the ROC curve of the score was 0.781. All nine patients with score 3 developed recurrence within 6 months after LT. Of 71 patients without vascular invasion, three patients with both tumor number >3 and NLR≥3 developed recurrence within 14 months after LT while the 5-year DFS and OS for patients with a score of 0 or 1 were 68.1% and 62.8%, respectively.
CONCLUSIONS/SIGNIFICANCE: Preoperative elevated NLR significantly increases the risk of recurrence in patients underwent LT for HCC. Patients with both NLR≥3 and tumor number >3 are not a good indication for LT. Our score model may aid in the selection of patients that would most benefit from transplantation for HCC.
中性粒细胞与淋巴细胞比值(NLR)已被提出用于预测肝细胞癌(HCC)的预后。然而,这些截断值是经验性的。我们确定了预测 HCC 患者肝移植(LT)后复发的最佳截断值,并进一步建立了基于 NLR 的评分模型。
方法/主要发现:我们分析了 101 例乙型肝炎病毒相关 HCC 患者 LT 后的结果。通过单因素分析评估了肿瘤复发的术前危险因素。通过 ROC 分析,将 NLR≥3 视为升高。NLR 升高的患者无疾病生存率(DFS)和总生存率(OS)明显低于 NLR 正常的患者(5 年 DFS 和 OS 分别为 28.5%和 19.5% vs. 64.9%和 61.8%;P<0.001)。单因素分析显示肿瘤大小>5cm、肿瘤数量>3、大血管侵犯、AFP≥400μg/L、NLR≥3 和 HBV-DNA 水平>5log10 拷贝/ml 是 DFS 的术前预测因素。Cox 回归分析显示大血管侵犯、肿瘤数量和高 NLR 是独立的预后因素。然后,我们根据多因素分析建立了术前预后评分。每个因素的评分均为 1。评分的 ROC 曲线下面积为 0.781。评分 3 分的 9 例患者在 LT 后 6 个月内均发生复发。在 71 例无血管侵犯的患者中,3 例肿瘤数量>3 且 NLR≥3 的患者在 LT 后 14 个月内复发,而评分 0 或 1 的患者 5 年 DFS 和 OS 分别为 68.1%和 62.8%。
结论/意义:术前 NLR 升高显著增加了 HCC 患者 LT 后复发的风险。NLR≥3 且肿瘤数量>3 的患者不适合 LT。我们的评分模型可能有助于选择最受益于 HCC 移植的患者。