Department of Internal Medicine, Subdivision of Rheumatology, Maastricht University Medical Center, P, Debyelaan 25 Postbus 5800, 6202 AZ Maastricht, The Netherlands.
Arthritis Res Ther. 2011;13(5):242. doi: 10.1186/ar3375. Epub 2011 Sep 30.
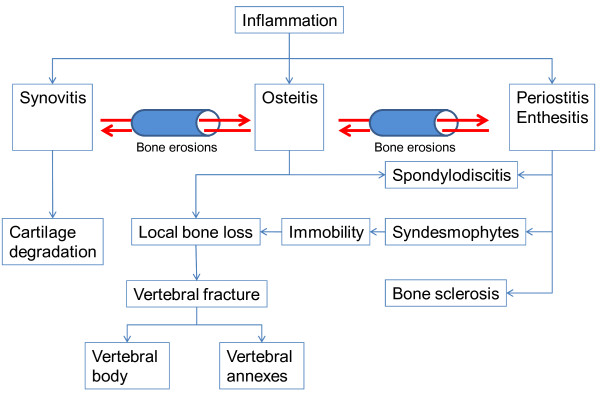
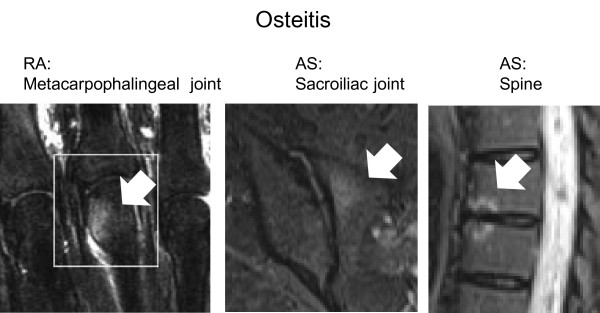
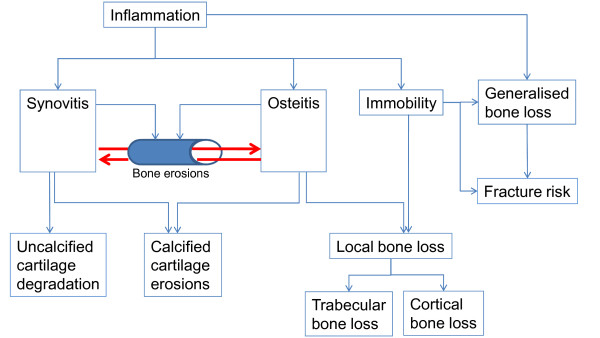
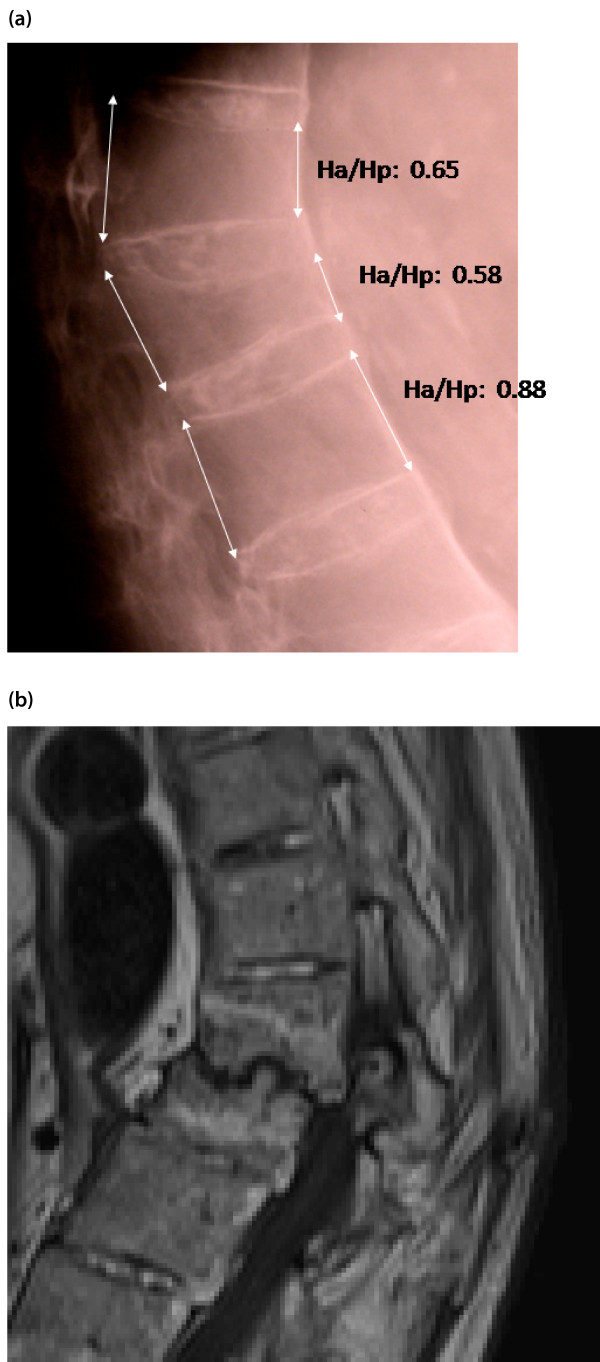
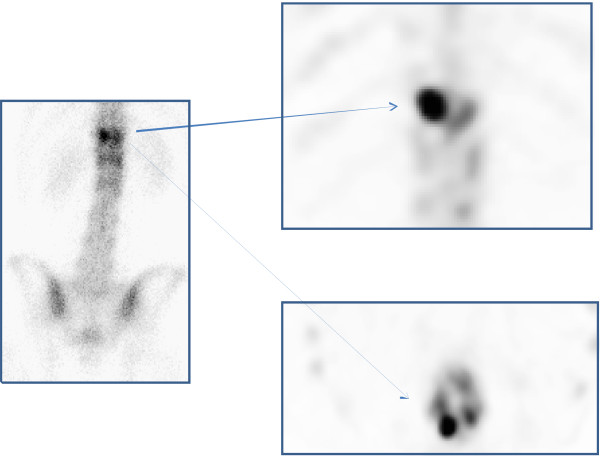
The concept of osteoimmunology is based on growing insight into the links between the immune system and bone at the anatomical, vascular, cellular, and molecular levels. In both rheumatoid arthritis (RA) and ankylosing spondylitis (AS), bone is a target of inflammation. Activated immune cells at sites of inflammation produce a wide spectrum of cytokines in favor of increased bone resorption in RA and AS, resulting in bone erosions, osteitis, and peri-inflammatory and systemic bone loss. Peri-inflammatory bone formation is impaired in RA, resulting in non-healing of erosions, and this allows a local vicious circle of inflammation between synovitis, osteitis, and local bone loss. In contrast, peri-inflammatory bone formation is increased in AS, resulting in healing of erosions, ossifying enthesitis, and potential ankylosis of sacroiliac joints and intervertebral connections, and this changes the biomechanical competence of the spine. These changes in bone remodeling and structure contribute to the increased risk of vertebral fractures (in RA and AS) and non-vertebral fractures (in RA), and this risk is related to severity of disease and is independent of and superimposed on background fracture risk. Identifying patients who have RA and AS and are at high fracture risk and considering fracture prevention are, therefore, advocated in guidelines. Local peri-inflammatory bone loss and osteitis occur early and precede and predict erosive bone destruction in RA and AS and syndesmophytes in AS, which can occur despite clinically detectable inflammation (the so-called 'disconnection'). With the availability of new techniques to evaluate peri-inflammatory bone loss, osteitis, and erosions, peri-inflammatory bone changes are an exciting field for further research in the context of osteoimmunology.
骨免疫学的概念基于对免疫系统和骨骼在解剖学、血管、细胞和分子水平上的联系的深入了解。在类风湿关节炎(RA)和强直性脊柱炎(AS)中,骨骼都是炎症的靶点。炎症部位的活化免疫细胞产生广泛的细胞因子,有利于 RA 和 AS 中骨吸收的增加,导致骨侵蚀、骨炎和炎症周围及全身性骨丢失。RA 中的炎症周围骨形成受损,导致侵蚀无法愈合,从而允许滑膜炎、骨炎和局部骨丢失之间形成局部恶性循环。相比之下,AS 中的炎症周围骨形成增加,导致侵蚀愈合、骨化附着点炎和骶髂关节和椎间连接潜在强直,并改变脊柱的生物力学能力。这些骨重塑和结构的变化导致椎体骨折(在 RA 和 AS 中)和非椎体骨折(在 RA 中)的风险增加,并且这种风险与疾病的严重程度有关,并且独立于和叠加于背景骨折风险。因此,指南提倡识别患有 RA 和 AS 且骨折风险高的患者,并考虑预防骨折。局部炎症周围骨丢失和骨炎发生较早,并且在 RA 和 AS 中的侵蚀性骨破坏和 AS 中的骨桥之前发生,并预测其发生,尽管临床上可检测到炎症(所谓的“脱钩”)。随着评估炎症周围骨丢失、骨炎和侵蚀的新技术的出现,炎症周围骨变化是骨免疫学领域进一步研究的一个令人兴奋的领域。