The Heart Center of Chonnam National University Hospital, Gwangju, Korea.
Korean J Intern Med. 2011 Sep;26(3):294-303. doi: 10.3904/kjim.2011.26.3.294. Epub 2011 Sep 13.
BACKGROUND/AIMS: A controversy exists about which statin is preferable for patients with acute myocardial infarction (AMI), and clinical impacts of different statins according to lipophilicity have not been established.
The 1,124 patients with AMI included in the present study were divided into hydrophilic- and lipophilic-statin groups. In-hospital complications (defined as death, cardiogenic shock, ventricular arrhythmia, infection, bleeding, and renal insufficiency, and other fatal arrhythmias), major adverse cardiac events (MACE), all-cause death, re-myocardial infarction, re-percutaneous coronary intervention (re-PCI), and surgical revascularization were analyzed during a 1-year clinical follow-up.
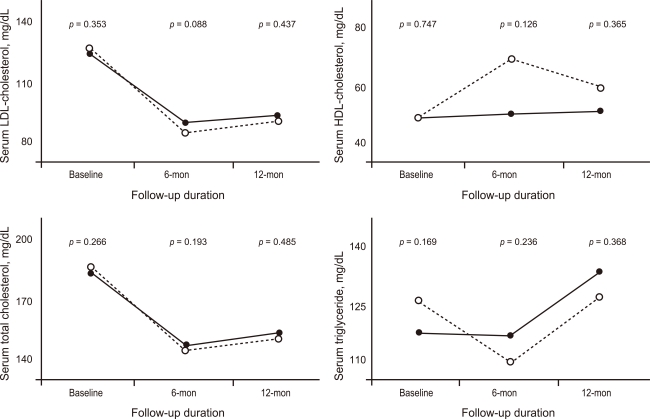
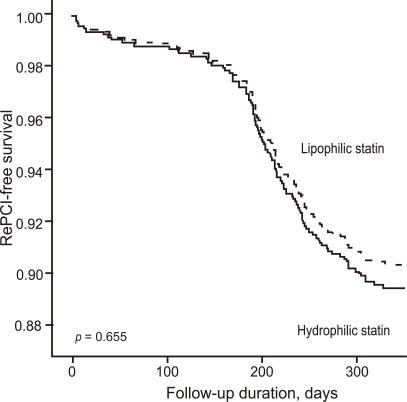
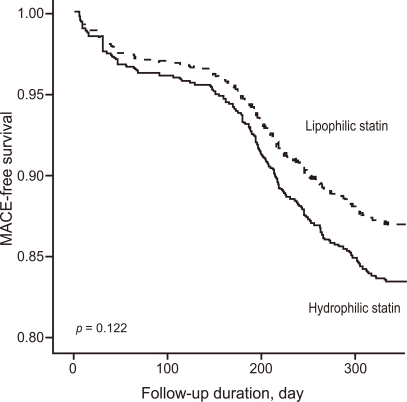
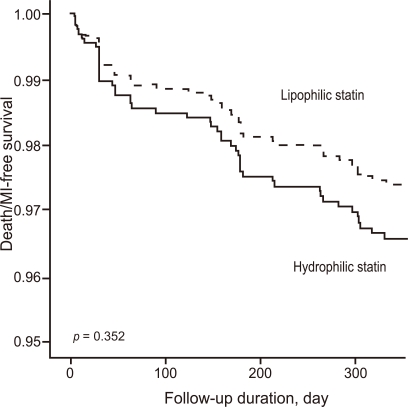
Baseline characteristics were similar between the two groups, and in-hospital complication rates showed no between-group differences (11.7% vs. 12.8%, p = 0.688). Although MACE at the 1- and 6-month clinical follow-ups occurred more in hydrophilic statin group I (1 month: 10.0% vs. 4.4%, p = 0.001; 6 month: 19.9% vs. 14.2%, p = 0.022), no significant difference in MACE was observed at the 1-year follow-up (21.5% vs. 17.9%, p = 0.172). Both statin groups showed similar efficacy for reducing serum lipid concentrations. A Cox-regression analysis showed that the use of a hydrophilic statin did not predict 1-year MACE, all-cause death, AMI, or re-PCI.
Although short-term cardiovascular outcomes were better in the lipophilic-statin group, 1-year outcomes were similar in patients with AMI who were administered hydrophilic and lipophilic statins. In other words, the type of statin did not influence 1-year outcomes in patients with AMI.
背景/目的:对于急性心肌梗死(AMI)患者,哪种他汀类药物更优存在争议,并且根据亲脂性确定不同他汀类药物的临床影响尚未确定。
本研究纳入的 1124 例 AMI 患者分为亲水性他汀类药物组和疏水性他汀类药物组。在住院期间的并发症(定义为死亡、心源性休克、室性心律失常、感染、出血和肾功能不全以及其他致命性心律失常)、主要不良心脏事件(MACE)、全因死亡、再心肌梗死、再次经皮冠状动脉介入治疗(再 PCI)和手术血运重建在 1 年临床随访期间进行分析。
两组患者的基线特征相似,住院并发症发生率无组间差异(11.7%比 12.8%,p = 0.688)。尽管在 1 个月和 6 个月的临床随访中亲水性他汀类药物组 I 的 MACE 发生率更高(1 个月:10.0%比 4.4%,p = 0.001;6 个月:19.9%比 14.2%,p = 0.022),但在 1 年随访中 MACE 无显著差异(21.5%比 17.9%,p = 0.172)。两种他汀类药物均显示出相似的降低血清脂质浓度的疗效。Cox 回归分析显示,使用亲水性他汀类药物不能预测 1 年 MACE、全因死亡、AMI 或再 PCI。
尽管疏水性他汀类药物组的短期心血管结局更好,但在接受亲水性和疏水性他汀类药物治疗的 AMI 患者中,1 年结局相似。换句话说,他汀类药物的类型并未影响 AMI 患者的 1 年结局。