Department of Clinical Neuroscience, Institute of Psychiatry, King's College London, London, United Kingdom.
PLoS One. 2011;6(10):e25796. doi: 10.1371/journal.pone.0025796. Epub 2011 Oct 10.
It may be possible to thrombolyse ischaemic stroke (IS) patients up to 6 h by using penumbral imaging. We investigated whether a perfusion CT (CTP) mismatch can help to select patients for thrombolysis up to 6 h.
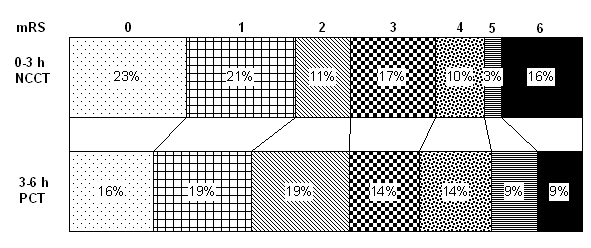
A cohort of 254 thrombolysed IS patients was studied. 174 (69%) were thrombolysed at 0-3 h by using non-contrast CT (NCCT), and 80 (31%) at 3-6 h (35 at 3-4.5 h and 45 at 4.5-6 h) by using CTP mismatch criteria. Symptomatic intracerebral haemorrhage (SICH), the mortality and the modified Rankin Score (mRS) were assessed at 3 months. Independent determinants of outcome in patients thrombolysed between 3 and 6 h were identified.
The baseline characteristics were comparable in the two groups. There were no differences in SICH (3% v 4%, p = 0.71), any ICH (7% v 9%, p = 0.61), or mortality (16% v 9%, p = 0.15) or mRS 0-2 at 3 months (55% v 54%, p = 0.96) between patients thrombolysed at 0-3 h (NCCT only) or at 3-6 h (CTP mismatch). There were no significant differences in outcome between patients thrombolysed at 3-4.5 h or 4.5-6 h. The NIHSS score was the only independent determinant of a mRS of 0-2 at 3 months (OR 0.89, 95% CI 0.82-0.97, p = 0.007) in patients treated using CTP mismatch criteria beyond 3 h.
The use of a CTP mismatch model may help to guide thrombolysis decisions up to 6 h after IS onset.
利用半暗带成像,有可能将缺血性卒中(IS)患者的溶栓时间延长至 6 小时。本研究旨在探讨灌注 CT(CTP)不匹配是否有助于选择 6 小时内接受溶栓治疗的患者。
研究纳入了 254 例接受溶栓治疗的 IS 患者。174 例(69%)在发病后 0-3 小时内接受非增强 CT(NCCT)检查,80 例(31%)在 3-6 小时内接受 CTP 不匹配标准检查。在 3 个月时评估症状性颅内出血(SICH)、死亡率和改良 Rankin 量表(mRS)评分。确定在 3-6 小时内溶栓患者的结局的独立决定因素。
两组患者的基线特征相似。两组 SICH(3%比 4%,p=0.71)、任何 ICH(7%比 9%,p=0.61)、死亡率(16%比 9%,p=0.15)或 mRS 0-2 评分在 3 个月时(55%比 54%,p=0.96)无差异。在发病后 3-4.5 小时或 4.5-6 小时溶栓的患者之间,结局无显著差异。NIHSS 评分是使用 CTP 不匹配标准在 3 小时后治疗的患者 mRS 0-2 评分的唯一独立决定因素(OR 0.89,95%CI 0.82-0.97,p=0.007)。
在发病 6 小时内,使用 CTP 不匹配模型可能有助于指导溶栓决策。