Faculty of Health Sciences, University of Ottawa, Ottawa, Canada.
J Int AIDS Soc. 2011 Nov 3;14:52. doi: 10.1186/1758-2652-14-52.
Because men in Africa are less likely to access HIV/AIDS care than women, we aimed to determine if men have differing outcomes from women across a nationally representative sample of adult patients receiving combination antiretroviral therapy in Uganda.
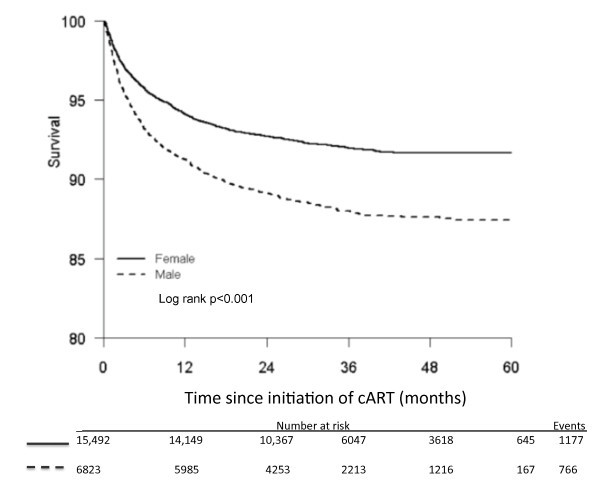
We estimated survival distributions for adult male and female patients using Kaplan-Meier, and constructed multivariable regressions to model associations of baseline variables with mortality. We assessed person-years of life lost up to age 55 by sex. To minimize the impact of patient attrition, we assumed a weighted 30% mortality rate among those lost to follow up.
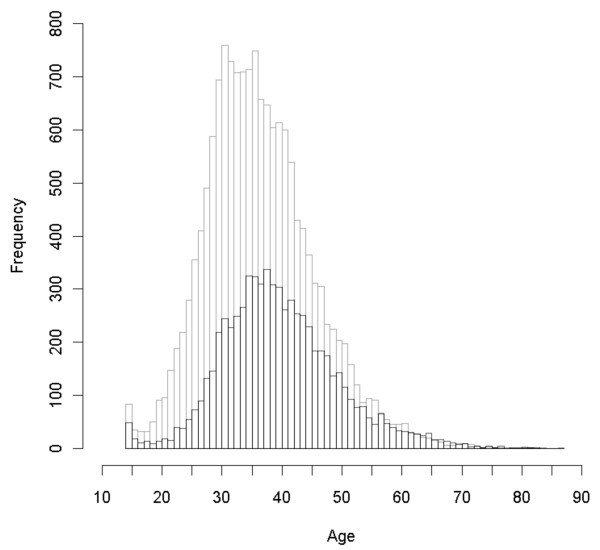
We included data from 22,315 adults receiving antiretroviral therapy. At baseline, men tended to be older, had lower CD4 baseline values, more advanced disease, had pulmonary tuberculosis and had received less treatment follow up (all at p < 0.001). Loss to follow up differed between men and women (7.5 versus 5.9%, p < 0.001). Over the period of study, men had a significantly increased risk of death compared with female patients (adjusted hazard ratio 1.43, 95% CI 1.31-1.57, p < 0.001). The crude mortality rate for males differed importantly from females (43.9, 95% CI 40.7-47.0/1000 person-years versus 26.9, 95% CI 25.4-28.5/1000 person years, p < 0.001). The probability of survival was 91.2% among males and 94.1% among females at 12 months. Person-years of life lost was lower for females than males (689.7 versus 995.9 per 1000 person-years, respectively).
In order to maximize the benefits of antiretroviral therapy, treatment programmes need to be gender sensitive to the specific needs of both women and men. Particular efforts are needed to enroll men earlier into care.
由于非洲男性获得艾滋病毒/艾滋病护理的机会比女性少,我们旨在确定在乌干达接受联合抗逆转录病毒治疗的成年患者中,是否存在全国代表性样本中男性与女性之间的不同结局。
我们使用 Kaplan-Meier 估计成年男性和女性患者的生存分布,并构建多变量回归模型,以对基线变量与死亡率的关联进行建模。我们根据性别评估了截止到 55 岁的预期寿命损失。为了最大限度地减少患者失访的影响,我们假设失访患者的死亡率为 30%。
我们纳入了 22315 名接受抗逆转录病毒治疗的成年人的数据。在基线时,男性往往年龄较大,CD4 基线值较低,疾病更为晚期,患有肺结核且接受的治疗随访较少(所有 p<0.001)。男性和女性的失访率不同(7.5%比 5.9%,p<0.001)。在研究期间,男性与女性患者相比,死亡风险显著增加(调整后的危险比 1.43,95%CI 1.31-1.57,p<0.001)。男性的粗死亡率与女性有显著差异(43.9,95%CI 40.7-47.0/1000人年与 26.9,95%CI 25.4-28.5/1000人年,p<0.001)。男性和女性在 12 个月时的生存率分别为 91.2%和 94.1%。女性的预期寿命损失低于男性(分别为 689.7 比 995.9/1000 人年)。
为了使抗逆转录病毒治疗的效益最大化,治疗方案需要对男女的具体需求具有性别敏感性。需要特别努力让男性更早地参与护理。