Hodgkinson Luqman Mushila, Abwalaba Roselyne Asiko, Arudo John, Barry Michele
Center for Innovation in Global Health.
Stanford University School of Medicine, Stanford University, Stanford, USA.
Medicine (Baltimore). 2020 May 22;99(21):e20328. doi: 10.1097/MD.0000000000020328.
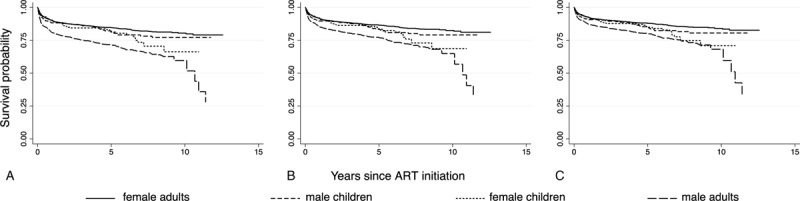
Evidence for why antiretroviral therapy (ART) outcomes differ by gender in developing countries has been inconclusive. In this first study to assess 10-year survival on ART in Kenya, our objective was to compare gender differences in survival for those who began ART as adults and as children. Kakamega County Referral Hospital (KCRH) is a tertiary rural hospital that has provided public ART to Kenyans since 2004. All patients enrolled in ART at KCRH who died between July 2004 and March 2017 and a sample of living patients were included in a survival analysis that bootstrapped sampled data. Case-cohort regressions identified adjusted hazard ratios. In total, 1360 patients were included in the study. Ten-year survival was 77% (95% confidence band [CB] 73-81%), significantly different for men (65%; 95% CB: 45-74%) and women (83%; 95% CB: 78-86%) who began therapy as adults. Ten-year survival was intermediate with no significant gender difference (76%; 95% CB: 69-81%) for patients who began therapy as children. Hazard of death was increased for men (hazard ratio [HR] 1.56; 95% confidence interval [CI] 1.13-2.17), infants (HR 2.87; 95% CI 1.44-5.74), patients with consistently poor clinic attendance (HR 3.94; 95% CI 3.19-4.86), and divorced patients (HR 2.25; 95% CI 1.19-4.25). Tuberculosis, diarrheal illnesses, human immunodeficiency virus (HIV) wasting syndrome, and malaria were leading causes of death. Survival was significantly lower for men than for women in all time periods, but only for patients who began therapy as adults, indicating against biological etiologies for the gender mortality difference.
在发展中国家,抗逆转录病毒疗法(ART)的治疗效果因性别而异,其原因尚无定论。在这项评估肯尼亚接受抗逆转录病毒疗法10年生存率的首次研究中,我们的目标是比较成年和儿童开始接受抗逆转录病毒疗法者的生存性别差异。卡卡梅加县转诊医院(KCRH)是一家乡村三级医院,自2004年以来一直为肯尼亚人提供公共抗逆转录病毒疗法。对2004年7月至2017年3月期间在KCRH登记接受抗逆转录病毒疗法且已死亡的所有患者以及一部分存活患者进行了生存分析,该分析对抽样数据进行了自抽样。病例队列回归确定了调整后的风险比。该研究共纳入了1360名患者。10年生存率为77%(95%置信区间[CB]为73 - 81%),成年开始接受治疗的男性(65%;95% CB:45 - 74%)和女性(83%;95% CB:78 - 86%)的生存率存在显著差异。儿童开始接受治疗的患者10年生存率处于中等水平,无显著性别差异(76%;95% CB:69 - 81%)。男性(风险比[HR] 1.56;95%置信区间[CI] 1.13 - 2.17)、婴儿(HR 2.87;95% CI 1.44 - 5.74)、门诊出勤率一直较低的患者(HR 3.94;95% CI 3.19 - 4.86)以及离婚患者(HR 2.25;95% CI 1.19 - 4.25)的死亡风险增加。结核病、腹泻病、人类免疫缺陷病毒(HIV)消瘦综合征和疟疾是主要死因。在所有时间段内,男性的生存率均显著低于女性,但仅在成年开始接受治疗的患者中如此,这表明性别死亡率差异并非由生物学病因导致。