Department of Anesthesiology & Perioperative Care, University of California, Irvine 101 S City Drive, Orange, CA 92868, USA.
Crit Care. 2011;15(6):R278. doi: 10.1186/cc10562. Epub 2011 Nov 23.
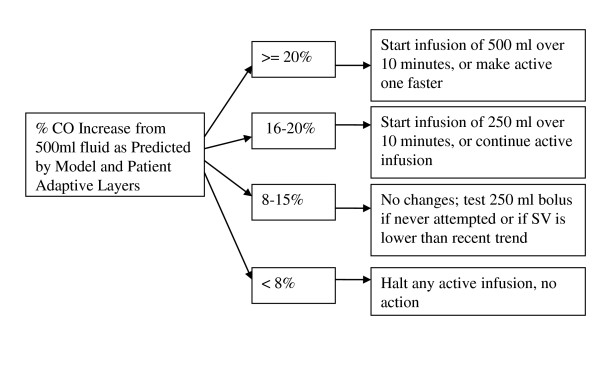
Dynamic predictors of fluid responsiveness have made automated management of fluid resuscitation more practical. We present initial simulation data for a novel closed-loop fluid-management algorithm (LIR, Learning Intravenous Resuscitator).
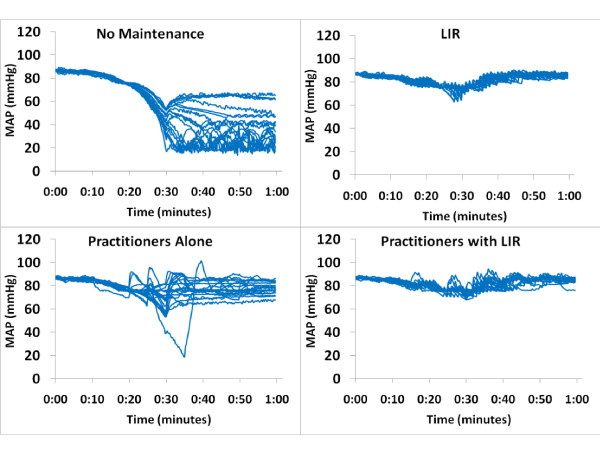
The performance of the closed-loop algorithm was tested in three phases by using a patient simulator including a pulse-pressure variation output. In the first phase, LIR was tested in three different hemorrhage scenarios and compared with no management. In the second phase, we compared LIR with 20 practicing anesthesiologists for the management of a simulated hemorrhage scenario. In the third phase, LIR was tested under conditions of noise and artifact in the dynamic predictor.
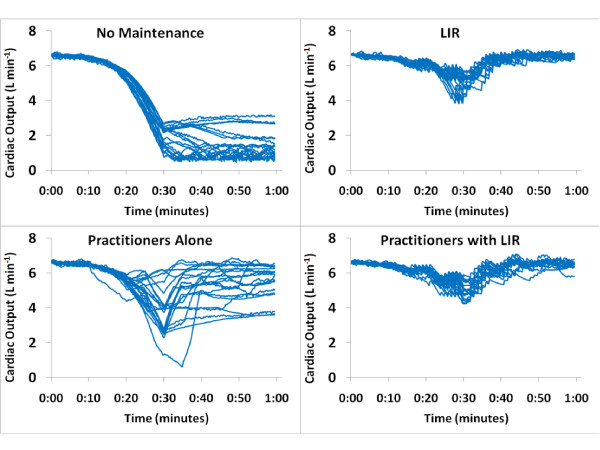
In the first phase, we observed a significant difference between the unmanaged and the LIR groups in moderate to large hemorrhages in heart rate (76 ± 8 versus 141 ± 29 beats/min), mean arterial pressure (91 ± 6 versus 59 ± 26 mm Hg), and cardiac output (CO; (6.4 ± 0.9 versus 3.2 ± 1.8 L/min) (P < 0.005 for all comparisons). In the second phase, LIR intervened significantly earlier than the practitioners (16.0 ± 1.3 minutes versus 21.5 ± 5.6 minutes; P < 0.05) and gave more total fluid (2,675 ± 244 ml versus 1,968 ± 644 ml; P < 0.05). The mean CO was higher in the LIR group than in the practitioner group (5.9 ± 0.2 versus 5.2 ± 0.6 L/min; P < 0.05). Finally, in the third phase, despite the addition of noise to the pulse-pressure variation value, no significant difference was found across conditions in mean, final, or minimum CO.
These data demonstrate that LIR is an effective volumetric resuscitator in simulated hemorrhage scenarios and improved physician management of the simulated hemorrhages.
液体反应性的动态预测指标使自动液体复苏管理更加实用。我们提出了一种新型闭环液体管理算法(LIR,学习静脉复苏器)的初步模拟数据。
使用包括脉压变异输出的患者模拟器,通过三个阶段测试闭环算法的性能。在第一阶段,在三种不同的出血情况下测试 LIR,并与无管理进行比较。在第二阶段,我们将 LIR 与 20 名执业麻醉师管理模拟出血情况进行比较。在第三阶段,在动态预测器存在噪声和伪影的情况下测试 LIR。
在第一阶段,我们观察到中度至大量出血时,未管理组和 LIR 组之间在心率(76±8 与 141±29 次/分钟)、平均动脉压(91±6 与 59±26 毫米汞柱)和心输出量(CO;(6.4±0.9 与 3.2±1.8 L/min)(所有比较均 P<0.005)方面存在显著差异。在第二阶段,LIR 干预的时间明显早于从业者(16.0±1.3 分钟与 21.5±5.6 分钟;P<0.05),并且给予更多的总液体(2675±244 ml 与 1968±644 ml;P<0.05)。LIR 组的平均 CO 高于从业者组(5.9±0.2 与 5.2±0.6 L/min;P<0.05)。最后,在第三阶段,尽管脉压变异值中添加了噪声,但在平均、最终或最小 CO 方面,各条件之间没有发现显著差异。
这些数据表明,LIR 是模拟出血情况下有效的容量复苏器,并改善了医生对模拟出血的管理。