Department of Trauma and Orthopedic Surgery, Berufsgenossenschaftliche Unfallklinik Murnau, Prof.-Küntscher-Str. 8, 82418 Murnau, Germany.
Scand J Trauma Resusc Emerg Med. 2011 Dec 9;19:73. doi: 10.1186/1757-7241-19-73.
Single-pass, whole-body computed tomography (pan-scan) remains a controversial intervention in the early assessment of patients with major trauma. We hypothesized that a liberal pan-scan policy is mainly an indicator of enhanced process quality of emergency care that may lead to improved survival regardless of the actual use of the method.
This retrospective cohort study included consecutive patients with blunt trauma referred to a trauma center prior to (2000 to 2002) and after (2002 to 2007) the introduction of a liberal single-pass pan-scan policy. The overall mortality between the two periods was compared and stratified according to the availability and actual use of the pan-scan. Logistic regression analysis was employed to adjust mortality estimates for demographic and injury-related independent variables.
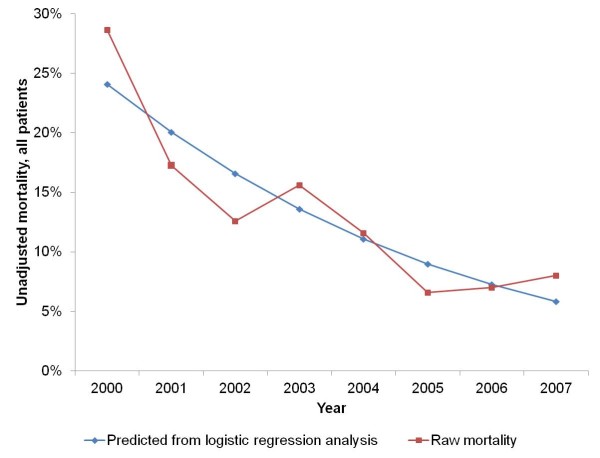
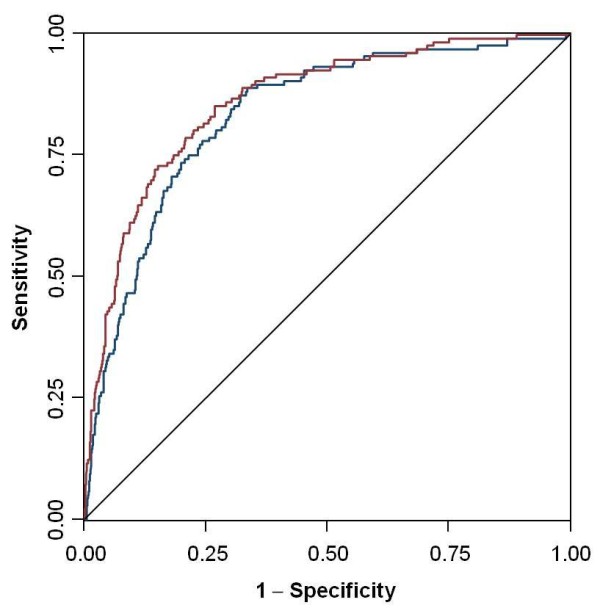
The study comprised 313 patients during the pre-pan-scan period, 223 patients after the introduction of the pan-scan policy but not undergoing a pan-scan and 608 patients undergoing a pan-scan. The overall mortality was 23.3, 14.8 and 7.9% (P < 0.001), respectively. By univariable logistic regression analysis, both the availability (odds ratio (OR) 0.57, 95% confidence interval (CI): 0.36 to 0.90) and the actual use of the pan-scan (OR 0.28, 95% CI: 0.19 to 0.42) were associated with a lower mortality. The final model contained the Injury Severity Score, the Glasgow Coma Scale, age, emergency department time and the use of the pan-scan. 2.7% of the explained variance in mortality was attributable to the use of the pan-scan. This contribution increased to 7.1% in the highest injury severity quartile.
In this study, a liberal pan-scan policy was associated with lower trauma mortality. The causal role of the pan-scan itself must be interpreted in the context of improved structural and process quality, is apparently moderate and needs further investigation with regard to the diagnostic yield and changes in management decisions. (The Pan-Scan for Trauma Resuscitation [PATRES] Study Group, ISRCTN35424832 and ISRCTN41462125).
单次全身计算机断层扫描(pan-scan)在评估严重创伤患者方面仍然是一种有争议的干预手段。我们假设,宽松的 pan-scan 政策主要是急诊护理过程质量提高的一个指标,这可能会导致生存率的提高,而与该方法的实际使用无关。
本回顾性队列研究纳入了在引入宽松的单次 pan-scan 政策之前(2000 年至 2002 年)和之后(2002 年至 2007 年)连续转诊至创伤中心的钝器创伤患者。比较了两个时期的总体死亡率,并根据 pan-scan 的可用性和实际使用情况进行分层。采用逻辑回归分析调整死亡率估计值,以适应人口统计学和损伤相关的独立变量。
该研究包括 313 名在 pan-scan 前期间接受治疗的患者,223 名在引入 pan-scan 政策但未进行 pan-scan 的患者,以及 608 名进行 pan-scan 的患者。总体死亡率分别为 23.3%、14.8%和 7.9%(P < 0.001)。单变量逻辑回归分析表明,pan-scan 的可用性(比值比(OR)0.57,95%置信区间(CI):0.36 至 0.90)和实际使用(OR 0.28,95%CI:0.19 至 0.42)均与死亡率降低相关。最终模型包含损伤严重程度评分、格拉斯哥昏迷评分、年龄、急诊时间和 pan-scan 的使用。死亡率中可归因于 pan-scan 使用的方差为 2.7%。在损伤严重程度最高的四分位数中,这一贡献增加到 7.1%。
在这项研究中,宽松的 pan-scan 政策与较低的创伤死亡率相关。pan-scan 本身的因果作用必须在结构和过程质量提高的背景下进行解释,其作用显然是适度的,并且需要进一步研究其诊断效果和管理决策的变化。(创伤复苏全扫描研究组,ISRCTN35424832 和 ISRCTN41462125)。