Dpt, of Clinical Medicine, "Sapienza" University of Rome, Rome, Italy.
BMC Infect Dis. 2011 Dec 14;11:341. doi: 10.1186/1471-2334-11-341.
The optimal therapeutic strategies for patients presenting with advanced disease at HIV-1 diagnosis are as yet incompletely defined.
All patients presenting at two outpatient clinics in 2000-2009 with an AIDS-defining clinical condition or a CD4+ T cell count < 200/μL at HIV-1 diagnosis were analyzed for the presence of combined immunovirological response, defined by the concomitant presence of an absolute number of CD4+ T cells > 200 cells/μL and a plasma HIV-1 RNA copy number < 50/mL after 12 months of HAART.
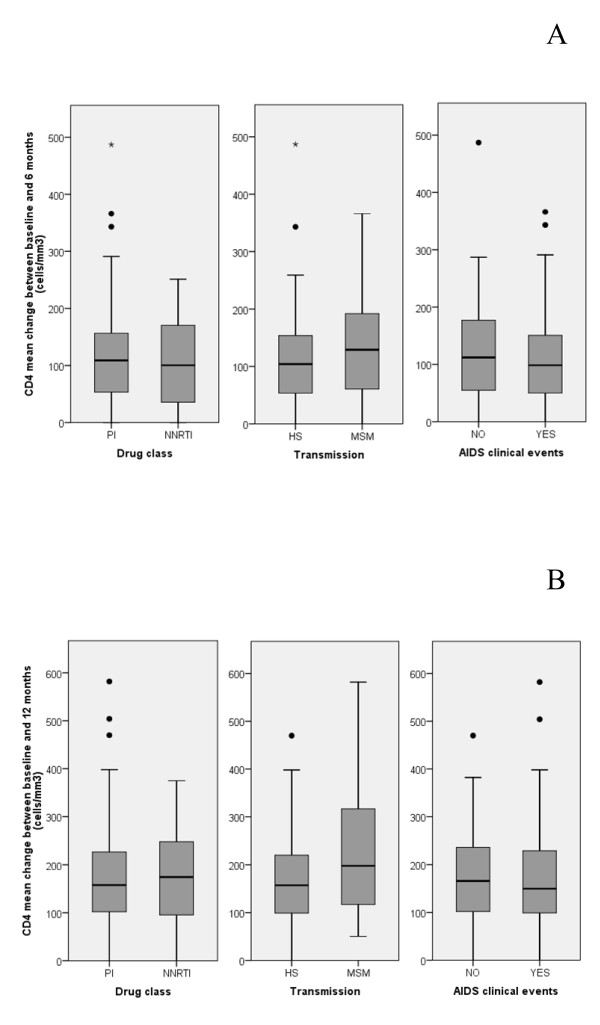
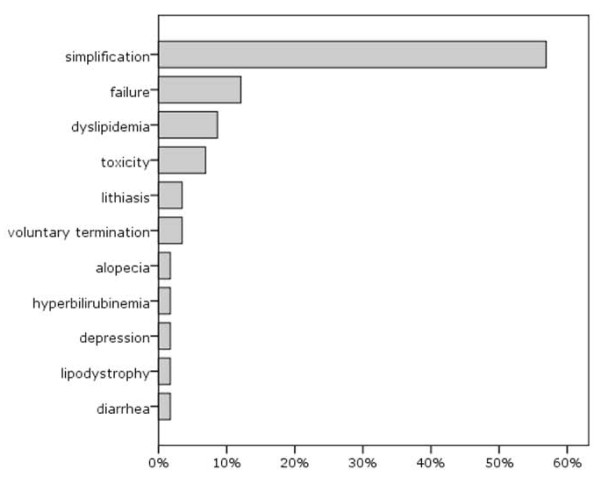
Among 102 evaluable patients, first-line regimens were protease inhibitors [PI]-based in 78 cases (77%) and efavirenz-based in 24 cases (23%). The overall response rate was 65% (95% CI: 55-74), with no differences by gender, age, nationality, route of transmission, hepatitis virus coinfections, presence of AIDS-defining clinical events, baseline HIV-1 viral load, or type of regimen (response rates with PI-based and efavirenz-based therapy: 63% and 71%, respectively, p = 0.474). Response rate was significantly better with higher baseline CD4+ T cell counts (78% with CD4+ ≥ 100/μL, compared to 50% with CD4+ < 100/μL; odds ratio: 3.5; 95% CI: 1.49-8.23, p = 0.003). Median time on first-line antiretroviral therapy was 24 months (interquartile range: 12-48). Switch to a second line treatment occurred in 57% of patients, mainly for simplification (57%), and was significantly more common with PI-based regimens [adjusted hazard ratios (AHR) with respect to efavirenz-based regimens: 3.88 for unboosted PIs (95% CI: 1.40-10.7, p = 0.009) and 4.21 for ritonavir-boosted PI (95% CI 1.7-10.4, p = 0.002)] and in older subjects (≥ 50 years) (AHR: 1.83; 95% CI: 1.02-3.31, p = 0.044). Overall mortality was low (3% after a median follow up of 48 months).
Our data indicate that a favorable immunovirological response is possible in the majority of naive patients presenting at HIV-1 diagnosis with AIDS or low CD4+ T cell counts, and confirm that starting HAART with a more compromised immune system may be associated with a delayed and sometimes partial immune recovery. Simpler regimens may be preferable in this particular population.
对于在人类免疫缺陷病毒 1 型(HIV-1)诊断时出现晚期疾病的患者,最佳治疗策略仍未完全确定。
分析了 2000 年至 2009 年在两个门诊就诊的所有患者,这些患者在 HIV-1 诊断时出现艾滋病定义性临床病症或 CD4+T 细胞计数<200/μL,且在接受高效抗逆转录病毒治疗(HAART)12 个月后,同时出现绝对 CD4+T 细胞数>200 个细胞/μL 和血浆 HIV-1 RNA 拷贝数<50/mL,以确定联合免疫病毒学反应的存在。
在 102 例可评估患者中,一线方案为蛋白酶抑制剂[PI]基础方案 78 例(77%)和依非韦伦基础方案 24 例(23%)。总体反应率为 65%(95%CI:55-74),性别、年龄、国籍、传播途径、肝炎病毒合并感染、艾滋病定义性临床事件、基线 HIV-1 病毒载量或方案类型无差异(PI 基础方案和依非韦伦基础方案的反应率分别为 63%和 71%,p=0.474)。基线 CD4+T 细胞计数较高时,反应率明显更好(CD4+≥100/μL 时为 78%,而 CD4+<100/μL 时为 50%;优势比:3.5;95%CI:1.49-8.23,p=0.003)。一线抗逆转录病毒治疗中位时间为 24 个月(四分位距:12-48)。57%的患者换用二线治疗,主要是为了简化治疗(57%),PI 基础方案换用二线治疗更为常见[未增强 PI 的调整后危险比(AHR)相对于依非韦伦基础方案:1.40-10.7,p=0.009)和利托那韦增强 PI(95%CI 1.7-10.4,p=0.002)],且在年龄较大的患者(≥50 岁)(AHR:1.83;95%CI:1.02-3.31,p=0.044)中更为常见。总体死亡率较低(中位随访 48 个月后为 3%)。
我们的数据表明,在大多数在 HIV-1 诊断时出现艾滋病或低 CD4+T 细胞计数的初治患者中,可能出现良好的免疫病毒学反应,并证实开始使用免疫功能更受损的 HAART 可能与免疫恢复延迟和有时不完全相关。在这一特定人群中,简单的方案可能更为理想。