University of Virginia Health System, Charlottesville, Virginia 22908-0300, USA.
Br J Surg. 2012 Mar;99(3):436-43. doi: 10.1002/bjs.7816. Epub 2012 Jan 11.
Disparities in the global availability of operating theatres, essential surgical equipment and surgically trained providers are profound. Although efforts are ongoing to increase surgical care and training, little is known about the surgical capacity in developing countries. The aim of this study was to create a baseline for surgical development planning at a national level.
A locally adapted World Health Organization survey was conducted in November 2010 to assess emergency and essential surgical capacity and volumes, with on-site interviews at 44 district and referral hospitals in Rwanda. Results were compiled for education and capacity development discussions with the Rwandan Ministry of Health and the Rwanda Surgical Society.
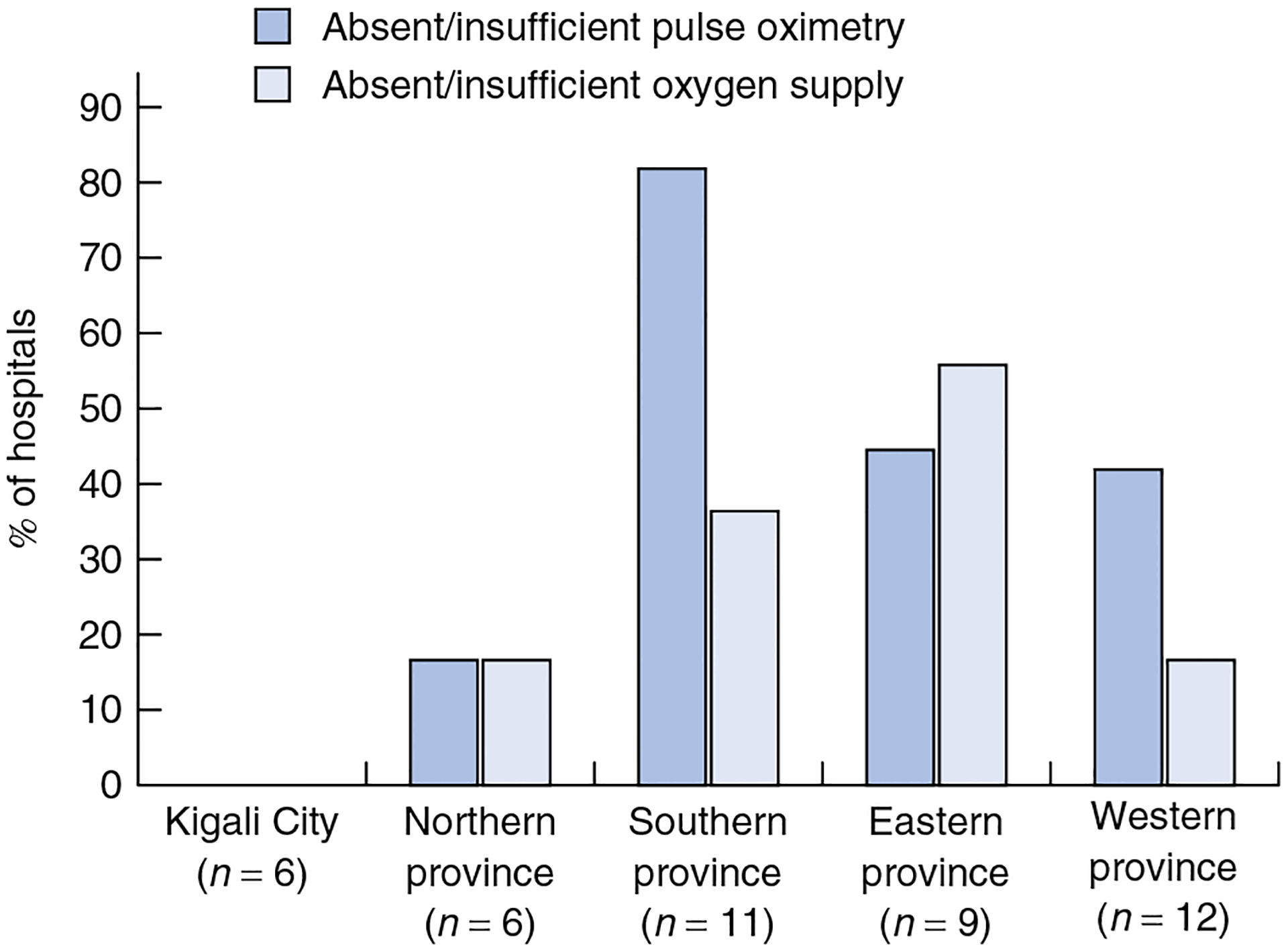
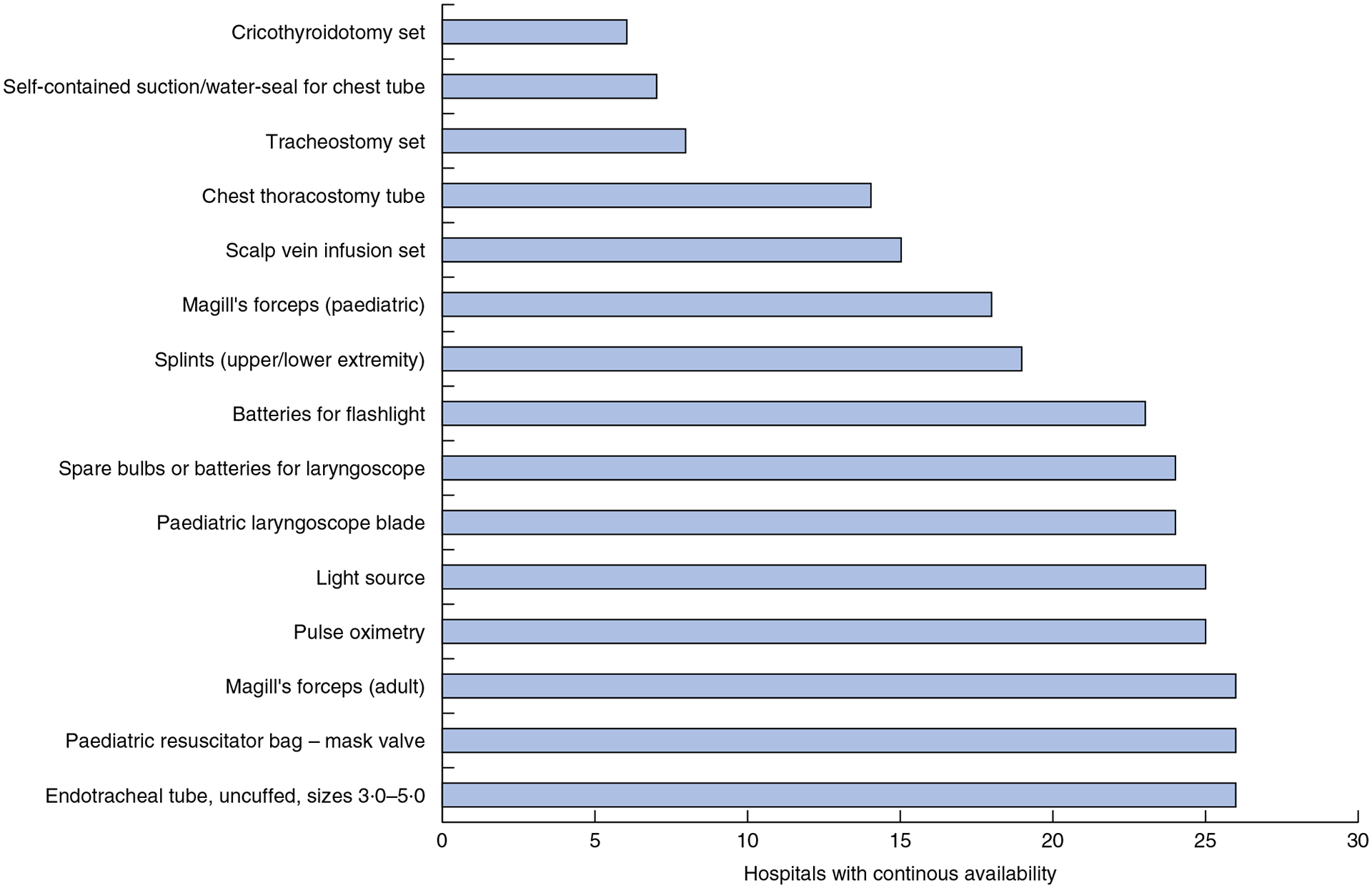
Among 10·1 million people, there were 44 hospitals and 124 operating rooms (1·2 operating rooms per 100,000 persons). There was a total of 50 surgeons practising full- or part-time in Rwanda (0·49 total surgeons per 100,000 persons). The majority of consultant surgeons worked in the capital (covering 10 per cent of the population). Anaesthesia was performed primarily by anaesthesia technicians, and six of 44 hospitals had no trained anaesthesia provider. Continuous availability of electricity, running water and generators was lacking in eight hospitals, and 19 reported an absence or shortage in the availability of pulse oximetry. Equipment for life-saving surgical airway procedures, particularly in children, was lacking. A dedicated emergency area was available in only 19 hospitals. In 2009 and 2010 over 80,000 surgical procedures (major and minor) were recorded annually in Rwanda.
A comprehensive countrywide assessment of surgical capacity in resource-limited settings found severe shortages in available resources. Immediate local feedback is a useful tool for creating a baseline of surgical capacity to inform country-specific surgical development.
全球各地手术间、基本外科设备和经过外科培训的医护人员的可及性差异很大。尽管正在努力增加外科护理和培训,但发展中国家的外科能力知之甚少。本研究旨在为国家一级的外科发展规划提供基线数据。
2010 年 11 月,采用世界卫生组织的当地改编版调查工具,对卢旺达 44 家区县级和转诊医院的紧急和基本外科能力和容量进行了评估,并进行了现场访谈。结果用于与卢旺达卫生部和卢旺达外科学会进行教育和能力发展讨论。
在 1010 万人中,有 44 家医院和 124 间手术室(每 10 万人 1.2 间手术室)。卢旺达共有 50 名全职或兼职外科医生(每 10 万人 0.49 名外科医生)。大多数顾问外科医生在首都工作(覆盖 10%的人口)。麻醉主要由麻醉技师进行,44 家医院中有 6 家没有经过培训的麻醉师。8 家医院缺乏持续的电力、自来水和发电机供应,19 家医院报告缺乏或短缺脉搏血氧仪。救命的外科气道处理设备,特别是儿童用设备,也严重短缺。只有 19 家医院设有专门的急救区。2009 年和 2010 年,卢旺达每年记录的外科手术量(大手术和小手术)超过 8 万例。
在资源有限的环境中对全国外科能力进行全面评估发现,可用资源严重短缺。当地即时反馈是创建外科能力基线的有用工具,可用于为特定国家的外科发展提供信息。