University Department of Surgery, Faculty of Medicine, University of Glasgow, Royal Infirmary, Glasgow, UK.
Br J Cancer. 2012 Feb 14;106(4):702-10. doi: 10.1038/bjc.2011.610. Epub 2012 Jan 12.
There is increasing evidence that the local and systemic inflammatory responses are associated with survival in oesophageal cancer. The aim of this study was to examine the relationship between tumour necrosis, tumour proliferation, local and systemic inflammation and microvessel density and survival in patients undergoing potentially curative resection of oesophageal adenocarcinoma.
The interrelationship between tumour necrosis, tumour proliferation, local inflammatory response (Klintrup-Makinen criteria, intra-tumoural CD8+ lymphocyte and macrophage infiltration), systemic inflammatory response (modified Glasgow Prognostic score (mGPS)), and microvessel density was examined in 121 patients undergoing potentially curative resection for oesophageal adenocarcinoma (including type I and II tumours of the gastro-oesophageal junction).
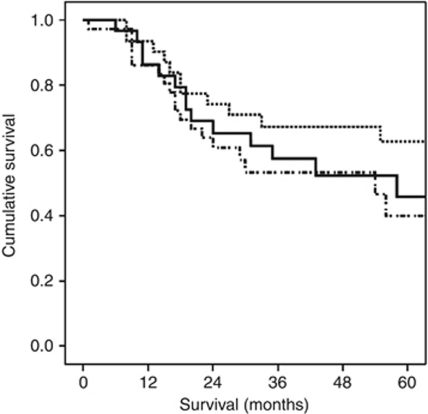
Tumour necrosis was not significantly associated with any tumour measure other than the degree of differentiation. On multivariate analysis, only age (HR 1.93, 95% CI 1.23-3.04, P=0.004), mGPS (HR 2.91, 95% CI 1.51-5.62, P=0.001), positive to total lymph node ratio (HR 2.38, 95% CI 1.60-3.52, P<0.001) and macrophage infiltration (HR 1.49, 95% CI 1.02-2.18, P=0.041) were independently associated with cancer-specific survival in oesophageal adenocarcinoma. Intra-tumoural macrophages were associated with tumour proliferation (P<0.001) and CD8+ lymphocytes infiltration (P<0.01).
The results of this study suggest that tumour necrosis does not link local and systemic inflammatory responses and is not significantly associated with survival. In contrast, tumour macrophage infiltration appears to have a central role in the proliferative activity and the coordination of the inflammatory cell infiltrate and is independently associated with poorer survival in patients with oesophageal adenocarcinoma.
越来越多的证据表明,局部和全身炎症反应与食管癌的生存有关。本研究旨在探讨肿瘤坏死、肿瘤增殖、局部炎症反应(克林特鲁普-马金宁标准、肿瘤内 CD8+淋巴细胞和巨噬细胞浸润)、全身炎症反应(改良格拉斯哥预后评分(mGPS))和微血管密度与接受食管腺癌根治性切除术患者的生存之间的关系。
在 121 例接受食管腺癌根治性切除术(包括胃食管交界处 I 型和 II 型肿瘤)的患者中,检查了肿瘤坏死与肿瘤其他指标(除分化程度外)之间的相互关系,包括肿瘤增殖、局部炎症反应(克林特鲁普-马金宁标准、肿瘤内 CD8+淋巴细胞和巨噬细胞浸润)、全身炎症反应(改良格拉斯哥预后评分(mGPS))和微血管密度。
肿瘤坏死与除分化程度以外的任何肿瘤指标均无显著相关性。多因素分析显示,仅年龄(HR 1.93,95%CI 1.23-3.04,P=0.004)、mGPS(HR 2.91,95%CI 1.51-5.62,P=0.001)、阳性总淋巴结比(HR 2.38,95%CI 1.60-3.52,P<0.001)和巨噬细胞浸润(HR 1.49,95%CI 1.02-2.18,P=0.041)与食管腺癌的癌症特异性生存独立相关。肿瘤内巨噬细胞与肿瘤增殖(P<0.001)和 CD8+淋巴细胞浸润(P<0.01)相关。
本研究结果表明,肿瘤坏死与局部和全身炎症反应无关,与生存无显著相关性。相反,肿瘤巨噬细胞浸润似乎在肿瘤的增殖活性和炎症细胞浸润的协调中起着核心作用,并且与食管腺癌患者的生存较差独立相关。