Mood Disorders Centre, University of Exeter, Exeter, EX4 4QG, UK.
Implement Sci. 2012 Jan 16;7:3. doi: 10.1186/1748-5908-7-3.
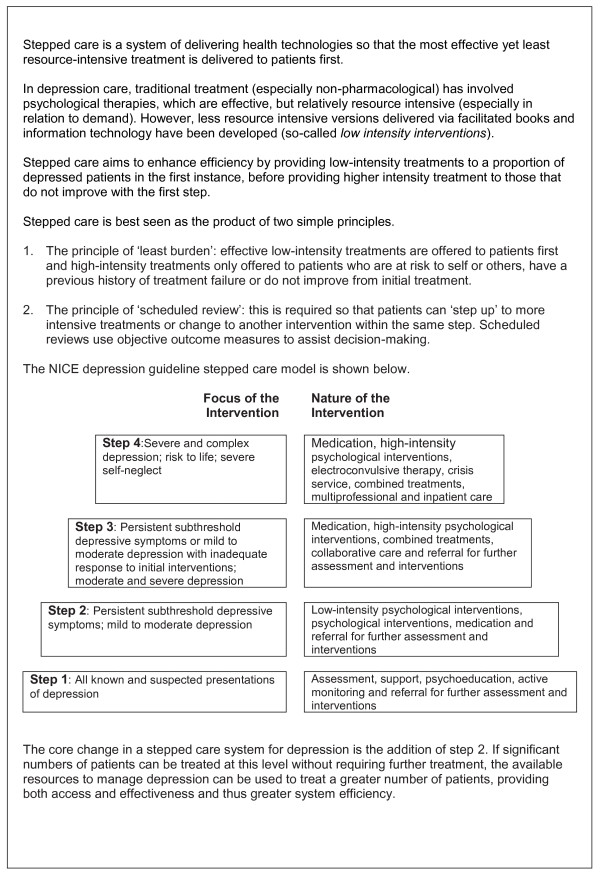
In the United Kingdom, clinical guidelines recommend that services for depression and anxiety should be structured around a stepped care model, where patients receive treatment at different 'steps,' with the intensity of treatment (i.e., the amount and type) increasing at each step if they fail to benefit at previous steps. There are very limited data available on the implementation of this model, particularly on the intensity of psychological treatment at each step. Our objective was to describe patient pathways through stepped care services and the impact of this on patient flow and management.
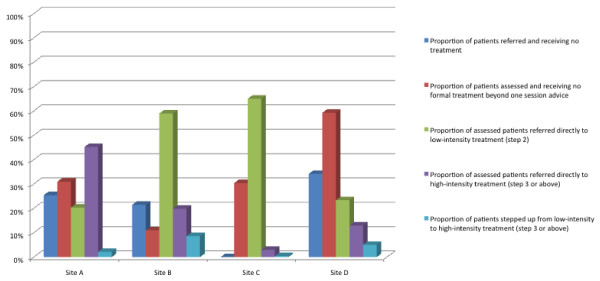
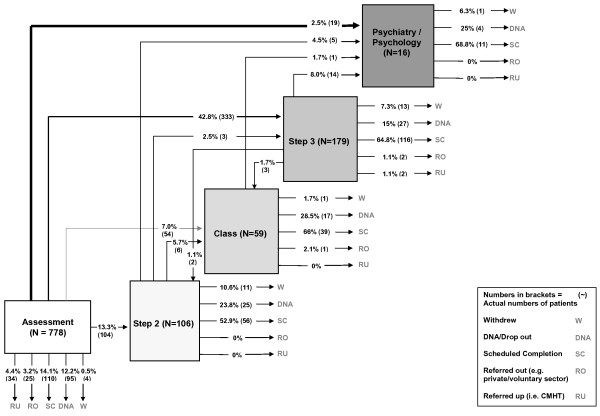
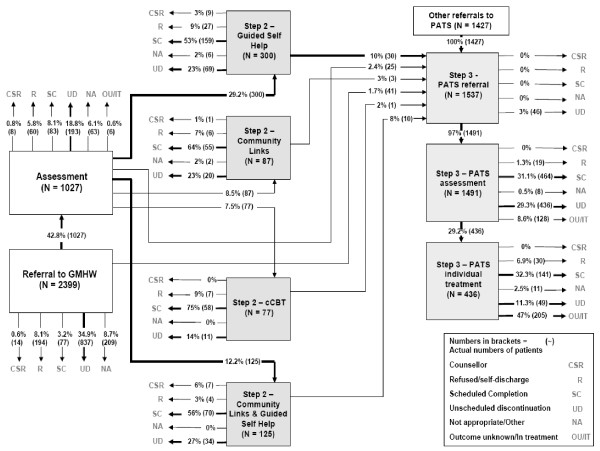
We recorded service design features of four National Health Service sites implementing stepped care (e.g., the types of treatments available and their links with other treatments), together with the actual treatments received by individual patients and their transitions between different treatment steps. We computed the proportions of patients accessing, receiving, and transiting between the various steps and mapped these proportions visually to illustrate patient movement.
We collected throughput data on 7,698 patients referred. Patient pathways were highly complex and very variable within and between sites. The ratio of low (e.g., self-help) to high-intensity (e.g., cognitive behaviour therapy) treatments delivered varied between sites from 22:1, through 2.1:1, 1.4:1 to 0.5:1. The numbers of patients allocated directly to high-intensity treatment varied from 3% to 45%. Rates of stepping up from low-intensity treatment to high-intensity treatment were less than 10%.
When services attempt to implement the recommendation for stepped care in the National Institute for Health and Clinical Excellence guidelines, there were significant differences in implementation and consequent high levels of variation in patient pathways. Evaluations driven by the principles of implementation science (such as targeted planning, defined implementation strategies, and clear activity specification around service organisation) are required to improve evidence on the most effective, efficient, and acceptable stepped care systems.
在英国,临床指南建议将抑郁症和焦虑症服务构建为阶梯式护理模式,根据该模式,患者在不同的“阶梯”接受治疗,如果在前一个阶梯未获益,治疗的强度(即治疗的数量和类型)会增加。关于该模式的实施情况,特别是每个阶梯的心理治疗强度,目前只有非常有限的数据。我们的目标是描述患者在阶梯式护理服务中的就诊路径,以及这对患者流程和管理的影响。
我们记录了实施阶梯式护理的四个英国国家医疗服务体系(NHS)站点的服务设计特征(例如,可用的治疗类型及其与其他治疗的联系),以及个体患者实际接受的治疗及其在不同治疗阶段之间的转移情况。我们计算了患者接受、接受和转移到不同治疗阶段的比例,并通过可视化的方式映射这些比例,以说明患者的流动情况。
我们收集了 7698 名转诊患者的吞吐量数据。患者的就诊路径非常复杂,且在各站点之间差异很大。站点之间提供的低强度(例如,自助)与高强度(例如,认知行为疗法)治疗的比例从 22:1 到 2.1:1、1.4:1 到 0.5:1 不等。直接分配到高强度治疗的患者人数从 3%到 45%不等。从低强度治疗升级到高强度治疗的比例不到 10%。
当服务尝试在英国国家卫生与临床优化研究所(NICE)指南中实施阶梯式护理的建议时,实施情况存在显著差异,导致患者就诊路径存在高度的变异性。需要采用实施科学的原则(例如,有针对性的规划、明确的实施策略以及明确的服务组织活动规范)进行评估,以提高最有效、最有效和最可接受的阶梯式护理系统的证据。