Department of Cardiac and Vascular Diseases, Jagiellonian University, Cracow, Poland.
Med Sci Monit. 2012 Feb;18(2):MT7-18. doi: 10.12659/msm.882452.
Significant atherosclerotic stenosis of internal carotid artery (ICA) origin is common (5-10% at ≥ 60 years). Intravascular ultrasound (IVUS) enables high-resolution (120 µm) plaque imaging, and IVUS-elucidated features of the coronary plaque were recently shown to be associated with its symptomatic rupture/thrombosis risk. Safety of the significant carotid plaque IVUS imaging in a large unselected population is unknown.
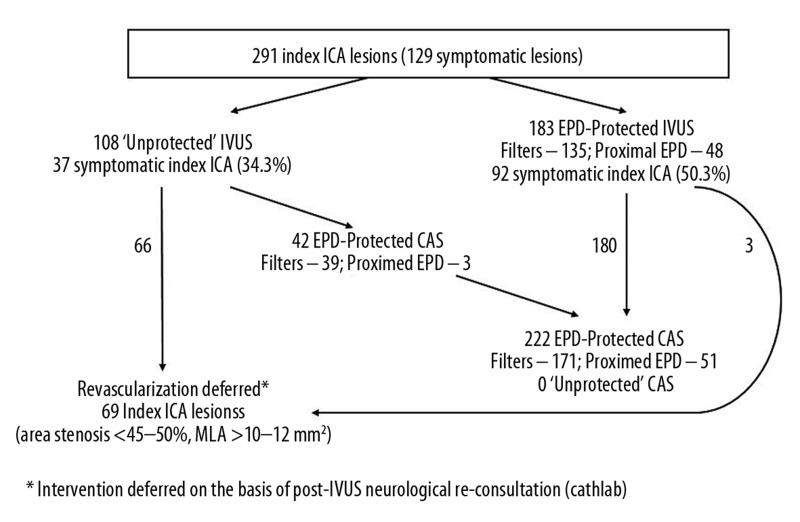
MATERIAL/METHODS: We prospectively evaluated the safety of embolic protection device (EPD)-assisted vs. unprotected ICA-IVUS in a series of consecutive subjects with ≥ 50% ICA stenosis referred for carotid artery stenting (CAS), including 104 asymptomatic (aS) and 187 symptomatic (S) subjects (age 47-83 y, 187 men). EPD use was optional for IVUS, but mandatory for CAS.
Evaluation was performed of 107 ICAs (36.8%) without EPD and 184 with EPD. Lesions imaged under EPD were overall more severe (peak-systolic velocity 2.97 ± 0.08 vs. 2.20 ± 0.08 m/s, end-diastolic velocity 1.0 ± 0.04 vs. 0.7 ± 0.03 m/s, stenosis severity of 85.7 ± 0.5% vs. 77.7 ± 0.6% by catheter angiography; mean ± SEM; p<0.01 for all comparisons) and more frequently S (50.0% vs. 34.6%, p=0.01). No ICA perforation or dissection, and no major stroke or death occurred. There was no IVUS-triggered cerebral embolization. In the procedures of (i) unprotected IVUS and no CAS, (ii) unprotected IVUS followed by CAS (filters - 39, flow reversal/blockade - 3), (iii) EPD-protected (filters - 135, flow reversal/blockade - 48) IVUS + CAS, TIA occurred in 1.5% vs. 4.8% vs. 2.7%, respectively, and minor stroke in 0% vs. 2.4% vs. 2.1%, respectively. EPD intolerance (on-filter ICA spasm or flow reversal/blockade intolerance) occurred in 9/225 (4.0%). IVUS increased the procedure duration by 7.27 ± 0.19 min.
Carotid IVUS is safe and, for the less severe lesions in particular, it may not require mandatory EPD use. High-risk lesions can be safely evaluated with IVUS under flow reversal/blockade.
颈内动脉(ICA)起源处的显著动脉粥样硬化狭窄很常见(≥60 岁时为 5-10%)。血管内超声(IVUS)可实现高分辨率(120μm)斑块成像,最近表明冠状动脉斑块的 IVUS 解析特征与斑块的症状性破裂/血栓形成风险相关。在未经选择的大人群中,使用有显著颈动脉斑块 IVUS 成像的安全性尚不清楚。
材料/方法:我们前瞻性评估了在因颈动脉支架置入术(CAS)而接受治疗的≥50%ICA 狭窄的连续患者系列中,使用或不使用栓塞保护装置(EPD)的 ICA-IVUS 的安全性,包括 104 例无症状(aS)和 187 例有症状(S)患者(年龄 47-83 岁,187 名男性)。IVUS 可选择使用 EPD,但 CAS 必须使用。
共评估了 107 个未使用 EPD 的 ICA(36.8%)和 184 个使用 EPD 的 ICA。EPD 下成像的病变总体更严重(峰值收缩速度 2.97±0.08 比 2.20±0.08m/s,舒张末期速度 1.0±0.04 比 0.7±0.03m/s,导管血管造影测量的狭窄严重程度 85.7±0.5%比 77.7±0.6%;均为平均值±SEM;所有比较的 p<0.01),且更常见于 S 组(50.0%比 34.6%,p=0.01)。未发生 ICA 穿孔或夹层,也未发生重大中风或死亡。没有 IVUS 触发的脑栓塞。在(i)未保护的 IVUS 且无 CAS、(ii)未保护的 IVUS 后行 CAS(过滤器-39 个,血流反转/阻断-3 个)、(iii)EPD 保护的(过滤器-135 个,血流反转/阻断-48 个)IVUS+CAS 这三种情况下,TIA 分别发生在 1.5%、4.8%和 2.7%,小中风分别发生在 0%、2.4%和 2.1%。EPD 不耐受(在过滤器上 ICA 痉挛或血流反转/阻断不耐受)发生在 9/225(4.0%)患者中。IVUS 将手术时间延长了 7.27±0.19 分钟。
颈动脉 IVUS 是安全的,对于较轻的病变,特别是可能不需要强制性使用 EPD。高危病变可以在血流反转/阻断下安全地使用 IVUS 进行评估。