INSERM U738, Paris, France.
BMJ. 2012 Feb 14;344:e813. doi: 10.1136/bmj.e813.
To compare estimates of intervention effects between single centre and multicentre randomised controlled trials with continuous outcomes.
Meta-epidemiological study.
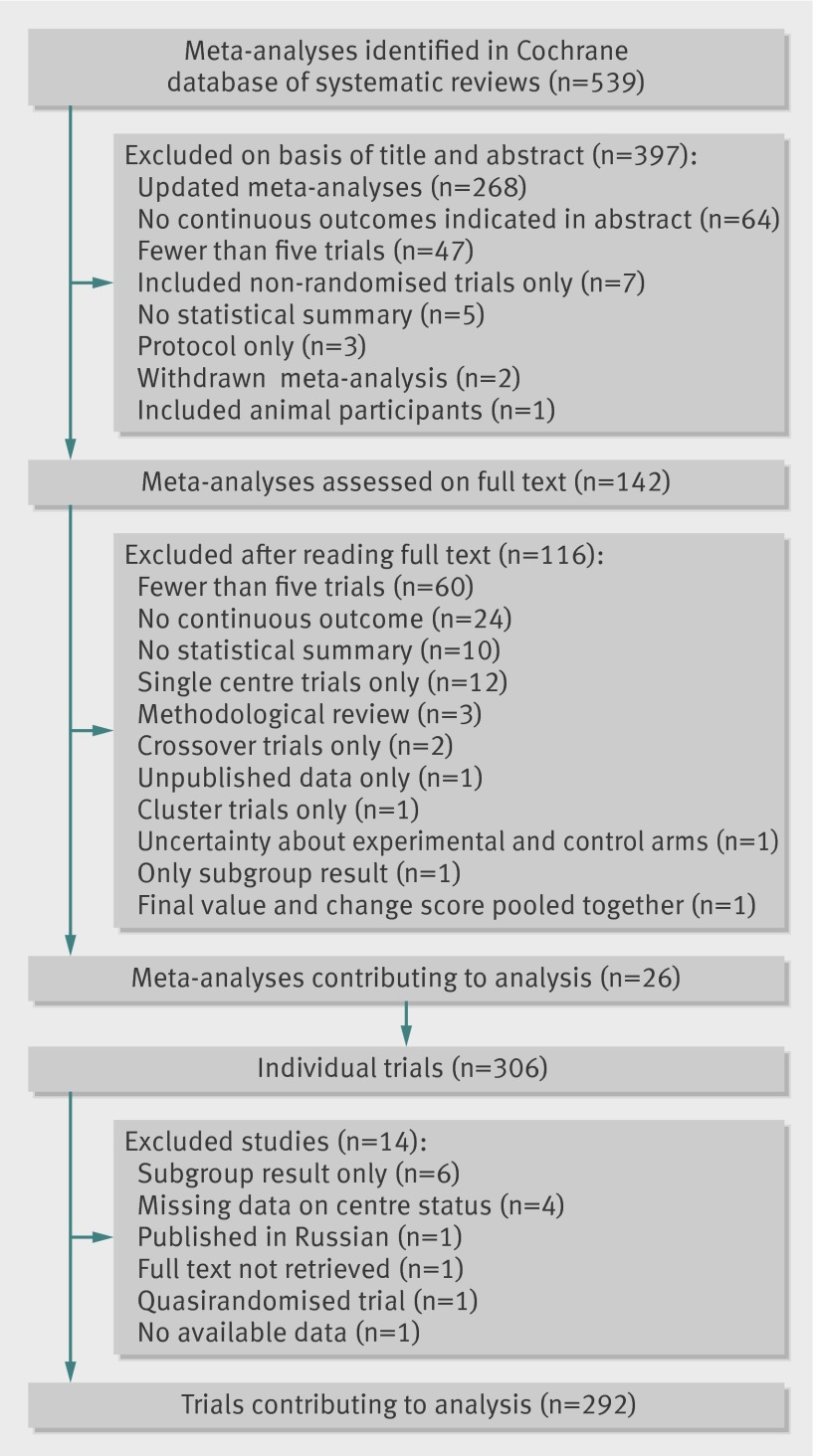
26 meta-analyses totalling 292 randomised controlled trials (177 single centre, 115 multicentre) with continuous outcomes published between January 2007 and January 2010 in the Cochrane database of systematic reviews.
Data were extracted on characteristics of trials, single or multicentre status, risk of bias using the risk of bias tool of the Cochrane Collaboration, and results.
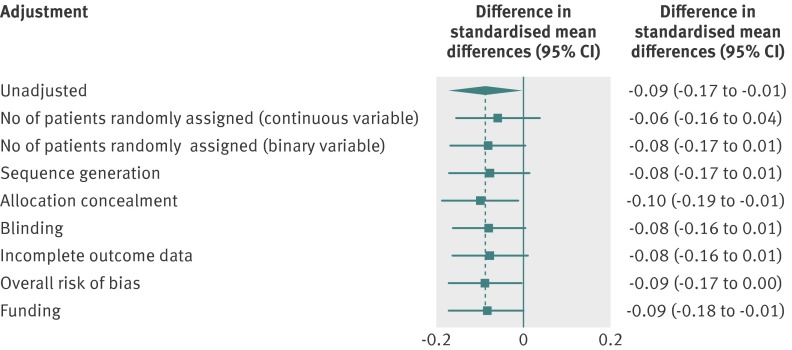
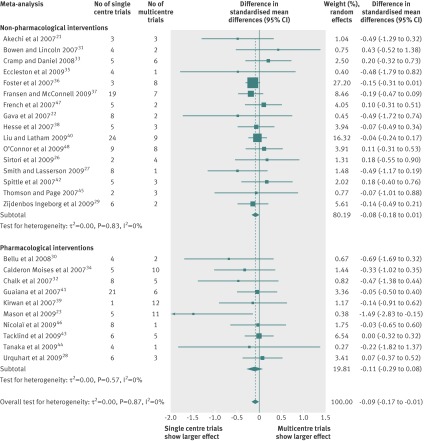
The intervention effects were estimated with standardised mean differences. For each meta-analysis, random effects meta-regression was used to estimate the difference in standardised mean differences between single centre and multicentre trials. Differences in standardised mean differences were then pooled across meta-analyses by a random-effects meta-analysis model. A combined difference in standardised mean differences of less than 0 indicated that single centre trials showed larger treatment effects, on average, than did multicentre trials. Because single centre trials may be more prone to publication bias and may have lower methodological quality than multicentre trials, sensitivity analyses were done with adjustment for sample size and domains of the risk of bias tool.
Single centre trials showed larger intervention effects than did multicentre trials (combined difference in standardised mean differences -0.09, 95% confidence interval -0.17 to -0.01, P=0.04), with low heterogeneity across individual meta-analyses (I(2)=0%, between meta-analyses variance τ(2)=0.00). Adjustment for sample size slightly attenuated the difference (-0.08, -0.17 to 0.01). Adjustment for risk of bias yielded similar estimates with wider confidence intervals, some of them crossing 0 (-0.09, -0.17 to 0.00 for overall risk of bias).
On average, single centre clinical trials with continuous outcomes showed slightly larger intervention effects than did multicentre trials. Further research is needed to investigate potential causes of these differences.
比较单中心和多中心随机对照试验(RCT)中连续结局的干预效果估计值。
Meta 流行病学研究。
2007 年 1 月至 2010 年 1 月期间在 Cochrane 系统评价数据库中发表的 26 项共 292 项 RCT(177 项单中心,115 项多中心)的 meta 分析,均为连续结局。
提取试验特征、单中心或多中心状态、Cochrane 协作风险偏倚工具评估的风险偏倚以及结果数据。
使用标准化均数差来估计干预效果。对于每个 meta 分析,采用随机效应 meta 回归来估计单中心和多中心试验的标准化均数差差异。然后通过随机效应 meta 分析模型,将各 meta 分析中的标准化均数差差异进行汇总。标准化均数差的综合差异小于 0 表示,单中心试验平均显示出更大的治疗效果,而多中心试验则显示出更小的治疗效果。由于单中心试验可能更容易受到发表偏倚的影响,且方法学质量可能低于多中心试验,因此进行了敏感性分析,以调整样本量和风险偏倚工具的各个领域。
单中心试验的干预效果大于多中心试验(标准化均数差综合差异-0.09,95%置信区间-0.17 至-0.01,P=0.04),个体 meta 分析之间的异质性较低(I²=0%,meta 分析间方差 τ²=0.00)。调整样本量后,差异略有减弱(-0.08,-0.17 至 0.01)。调整风险偏倚后,估计值置信区间较宽,其中一些值越过 0 点(总体风险偏倚为-0.09,-0.17 至 0.00)。
平均而言,具有连续结局的单中心临床试验的干预效果略大于多中心试验。需要进一步研究以探讨这些差异的潜在原因。