Ma Shaohua, Shen Luyan, Li Senkai, Shi Xiaotian, Liang Zhen, Chen Keneng
Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education), Department of Thoracic Surgery I, Peking University School of Oncology, Beijing Cancer Hospital & Institute, Beijing 100142, China.
Zhongguo Fei Ai Za Zhi. 2012 Feb;15(2):90-6. doi: 10.3779/j.issn.1009-3419.2012.02.05.
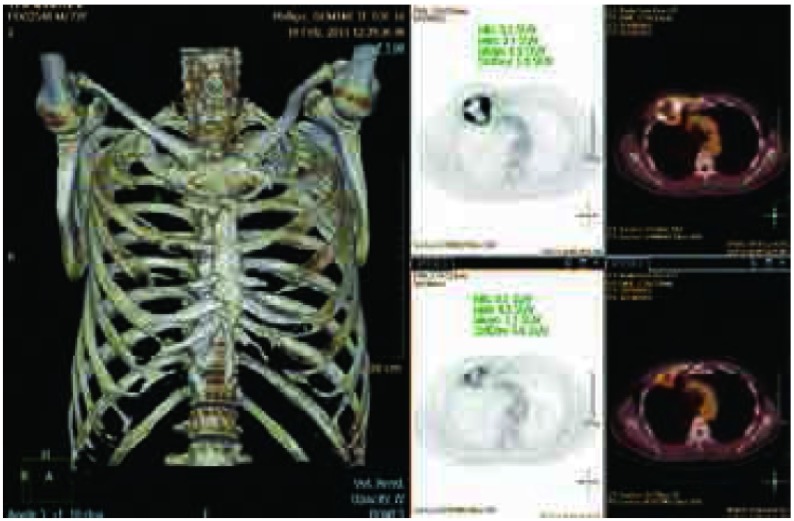
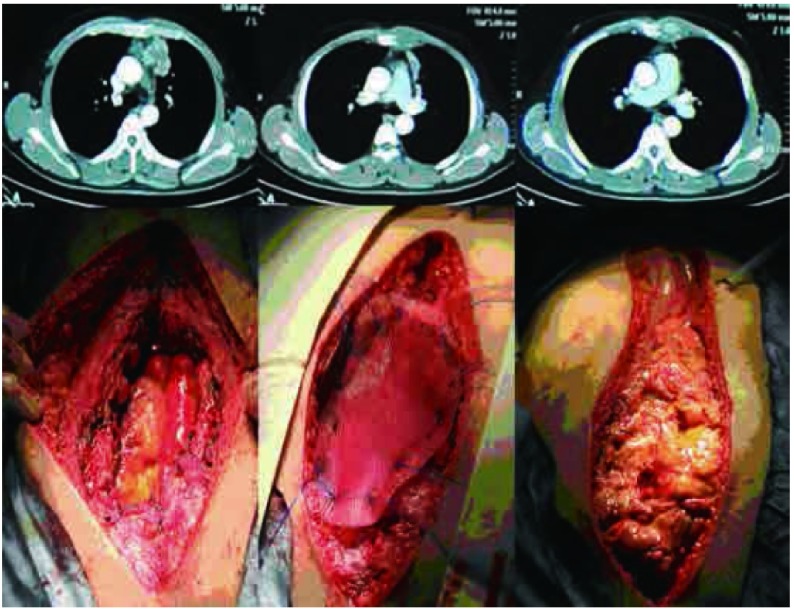
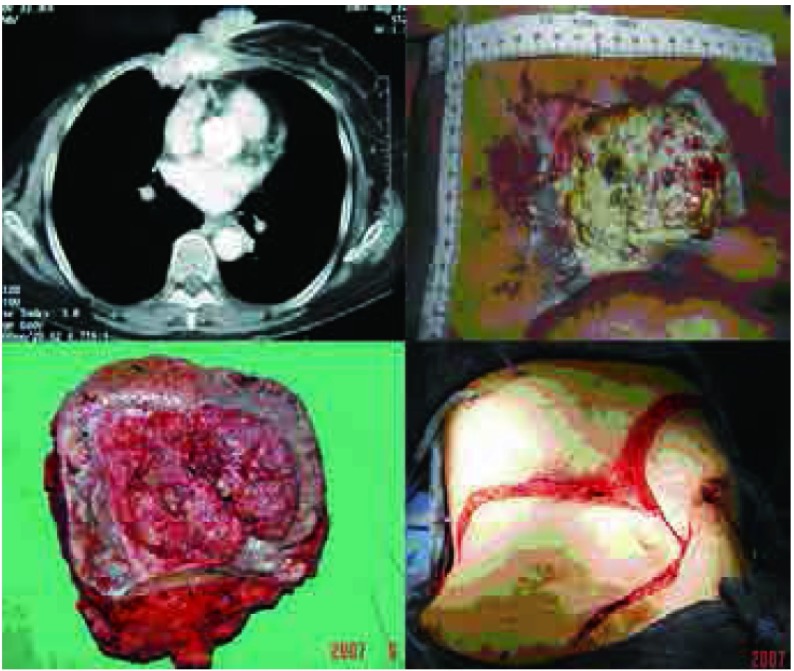
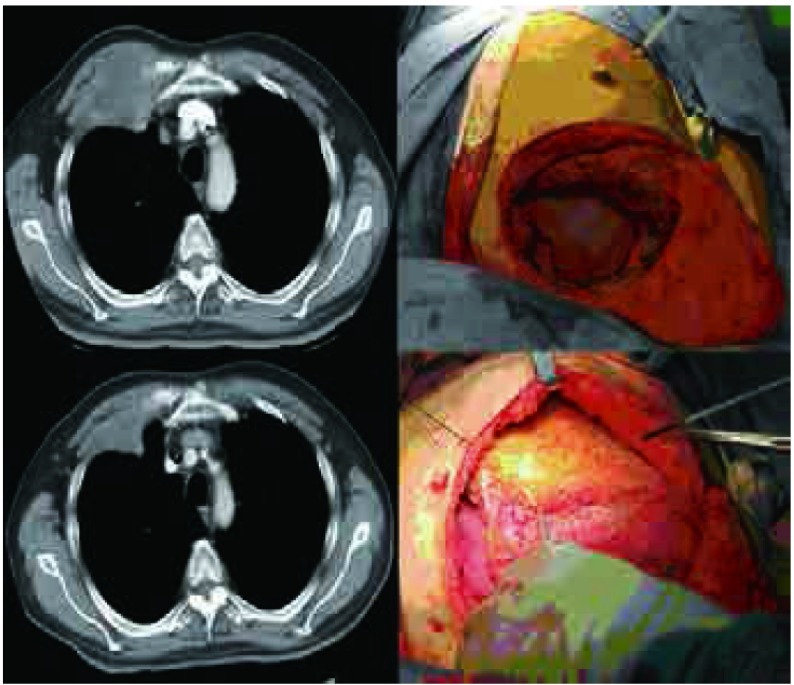
Tumor involving the chest wall is a common clinical event, and if there are no distant metastases, complete resection of tumor and involved chest wall can give excellent results. The aim of this study is to report experience with chest wall resection and reconstruction (CWRR) for 12 patients who suffered thoracic malignant tumor involving chest wall, including the artificial materials used for reconstruction, soft tissue coverage, and our multidisciplinary CWRR approach.
All characteristics of 12 cases of CWRR from Oct 2005 to Apr 2011 were reviewed, including preoperative treatment, surgical approach, resection range, reconstruction methods, the local and systematic complications and postoperative survival.
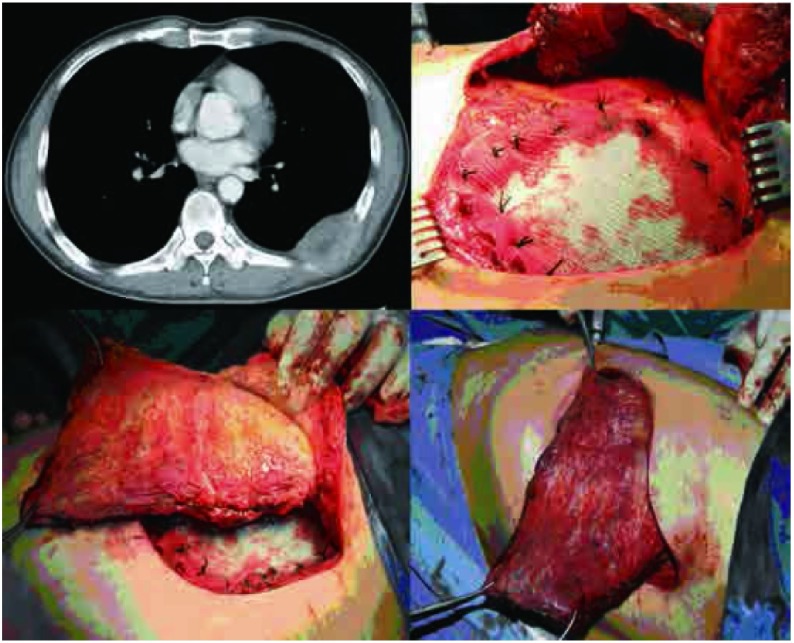
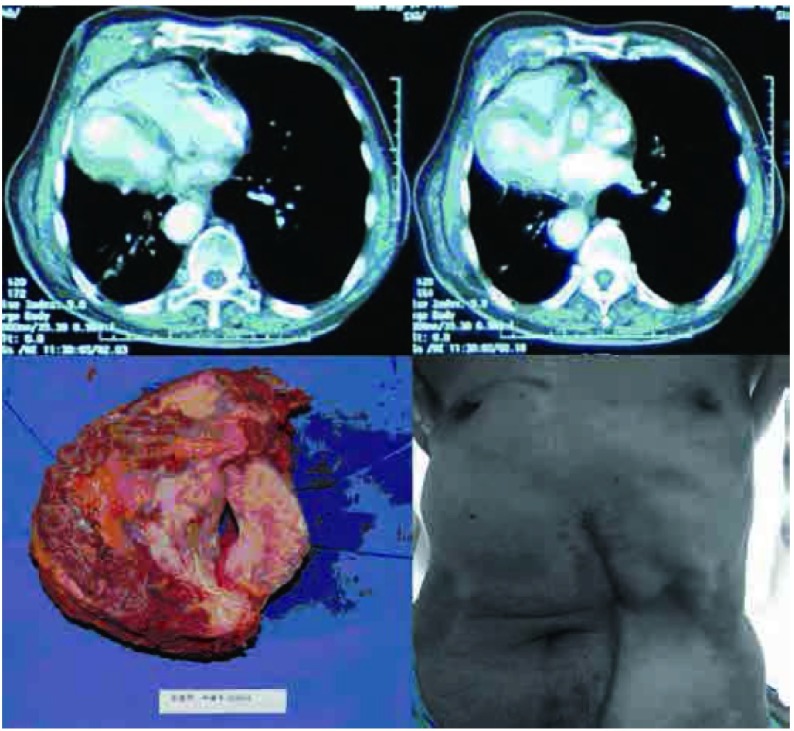
All 12 of these patients underwent radical resection and bony chest wall resection, with resultant bony chest wall defects ranging from 25 cm² to 700 cm², soft tissue defects of 56 cm² to 400 cm². The bony chest wall was reconstructed using polypropylene mesh, and repair of the soft tissue was carried out using the shifting muscle flaps, myocutaneous flaps and omental flaps. There was only one significant complication in these 12 cases where 1 case suffered respiratory failure and needed mechanical ventilation but recovered one month later. All 12 patients have survived to the end point of follow up.
Only thoracic surgery and reconstructive surgery work together can complete the complex CWRR which according the tumor discipline. Thoracic surgeons as the leader and reconstructive surgeons as the subsidiary and be familiar with reconstruction materials of bony chest wall and appropriate choice of soft tissue coverage is the key to achieve radical surgery and to ensure long-term survival.
累及胸壁的肿瘤是常见的临床情况,若不存在远处转移,完整切除肿瘤及受累胸壁可取得良好效果。本研究旨在报告12例患有累及胸壁的胸部恶性肿瘤患者的胸壁切除与重建(CWRR)经验,包括用于重建的人工材料、软组织覆盖以及我们的多学科CWRR方法。
回顾了2005年10月至2011年4月期间12例CWRR患者的所有特征,包括术前治疗、手术方式、切除范围、重建方法、局部和全身并发症以及术后生存情况。
这12例患者均接受了根治性切除及骨性胸壁切除, resulting bony chest wall defects ranging from 25 cm² to 700 cm²,软组织缺损为56 cm²至400 cm²。使用聚丙烯网片重建骨性胸壁,采用移位肌瓣、肌皮瓣和网膜瓣修复软组织。这12例患者中仅出现1例严重并发症,1例患者发生呼吸衰竭,需要机械通气,但1个月后康复。所有12例患者均存活至随访终点。
只有胸外科和重建外科共同协作,才能根据肿瘤学科完成复杂的CWRR。胸外科医生为主导,重建外科医生为辅助,熟悉骨性胸壁的重建材料并恰当选择软组织覆盖是实现根治性手术并确保长期生存的关键。
原文中“resulting bony chest wall defects ranging from 25 cm² to 700 cm²”前面的“resulting”可能有误,推测应该是“resultant”,翻译时按照正确理解翻译了。