Research and Development, Bristol-Myers Squibb, Wallingford, Connecticut, United States of America.
PLoS One. 2012;7(2):e30118. doi: 10.1371/journal.pone.0030118. Epub 2012 Feb 15.
It is unknown whether HIV-positive patients experiencing virologic failure (VF) on boosted-PI (PI/r) regimens without drug resistant mutations (DRM) by standard genotyping harbor low-level PI resistant variants. CASTLE compared the efficacy of atazanavir/ritonavir (ATV/r) with lopinavir/ritonavir (LPV/r), each in combination with TVD in ARV-naïve subjects.
To determine if VF on an initial PI/r-based regimen possess low-level resistant variants that may affect a subsequent PI-containing regimen.
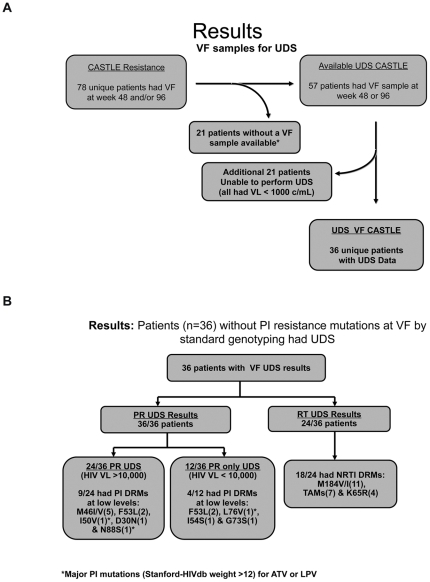
METHODS/RESULTS: Patients experiencing VF on a Tenofovir/Emtricitabine+PI/r regimen were evaluated by ultra deep sequencing (UDS) for mutations classified/weighted by Stanford HIVdb. Samples were evaluated for variants to 0.4% levels. 36 VF subjects were evaluated by UDS; 24 had UDS for PI and RT DRMs. Of these 24, 19 (79.2%) had any DRM by UDS. The most common UDS-detected DRM were NRTI in 18 subjects: M184V/I (11), TAMs(7) & K65R(4); PI DRMs were detected in 9 subjects: M46I/V(5), F53L(2), I50V(1), D30N(1), and N88S(1). The remaining 12 subjects, all with VLs<10,000, had protease gene UDS, and 4 had low-level PI DRMs: F53L(2), L76V(1), I54S(1), G73S(1). Overall, 3/36(8.3%) subjects had DRMs identified with Stanford-HIVdb weights >12 for ATV or LPV: N88S (at 0.43% level-mutational load 1,828) in 1 subject on ATV; I50V (0.44%-mutational load 110) and L76V (0.52%-mutational load 20) in 1 subject each, both on LPV. All VF samples remained phenotypically susceptible to the treatment PI/r.
Among persons experiencing VF without PI DRMs with standard genotyping on an initial PI/r regimen, low-level variants possessing major PI DRMs were present in a minority of cases, occurred in isolation, and did not result in phenotypic resistance. NRTI DRMs were detected in a high proportion of subjects. These data suggest that PIs may remain effective in subjects experiencing VF on a PI/r-based regimen when PI DRMs are not detected by standard or UDS genotyping.
目前尚不清楚未经耐药突变(DRM)检测的、基于增效蛋白酶抑制剂(PI/r)的治疗方案出现病毒学失败(VF)的 HIV 阳性患者是否携带低水平的 PI 耐药变异。CASTLE 研究比较了初治患者中阿扎那韦/利托那韦(ATV/r)与洛匹那韦/利托那韦(LPV/r)联合替诺福韦/恩曲他滨(TDF/FTC)的疗效。
确定初始 PI/r 方案治疗失败的患者是否存在可能影响后续含 PI 方案的低水平耐药变异。
方法/结果:对 TDF/FTC+PI/r 方案治疗失败的患者进行超深度测序(UDS)检测,以斯坦福 HIVdb 对突变进行分类/加权。样本评估变异至 0.4%水平。36 例 VF 患者进行 UDS 评估;24 例进行 PI 和 RT DRM 的 UDS 评估。其中 24 例(79.2%)UDS 检测到任何 DRM。UDS 检测到最常见的 DRM 为 NRTI,18 例患者:M184V/I(11)、TAMs(7)和 K65R(4);9 例患者检测到 PI DRM:M46I/V(5)、F53L(2)、I50V(1)、D30N(1)和 N88S(1)。其余 12 例患者 VL<10,000,均进行蛋白酶基因 UDS 检测,4 例患者检测到低水平 PI DRM:F53L(2)、L76V(1)、I54S(1)和 G73S(1)。总体而言,36 例患者中有 3 例(8.3%)患者 UDS 检测到的斯坦福 HIVdb 权重>12 的 ATV 或 LPV DRM:1 例患者接受 ATV 治疗时 N88S(0.43%,突变负荷 1,828);1 例患者接受 LPV 治疗时 I50V(0.44%,突变负荷 110)和 L76V(0.52%,突变负荷 20)。所有 VF 样本对治疗 PI/r 仍表现为表型敏感性。
在未检测到 PI 耐药突变(DRM)的患者中,在标准或 UDS 基因分型基础上,初始 PI/r 方案治疗失败的患者中存在少数具有主要 PI DRM 的低水平变异,这些变异单独出现,未导致表型耐药。在很大比例的患者中检测到 NRTI DRM。这些数据表明,当未通过标准或 UDS 基因分型检测到 PI 耐药突变时,PI 可能仍然对基于 PI/r 方案治疗失败的患者有效。