Department of Surgical Sciences - Section of Anatomic Pathology and Cytopathology, University of Foggia, Viale Luigi Pinto 1, 71122 Foggia, Italy.
Infect Agent Cancer. 2012 Feb 29;7:4. doi: 10.1186/1750-9378-7-4.
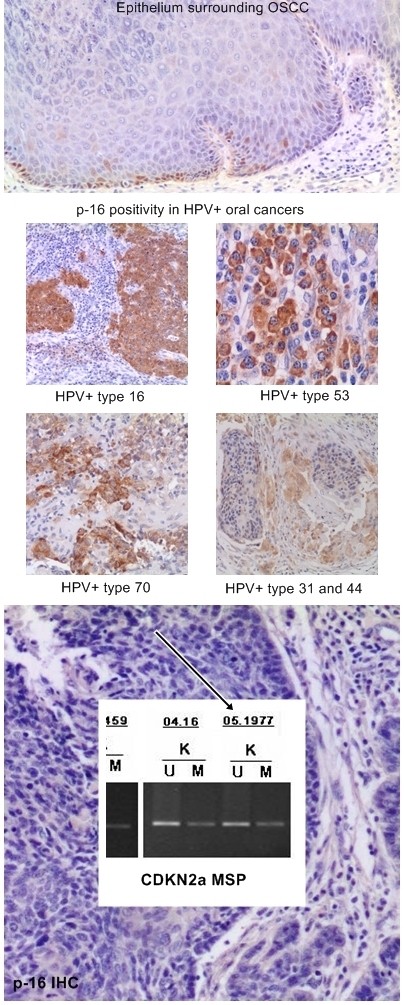
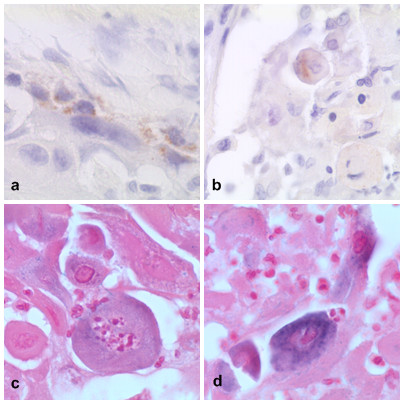
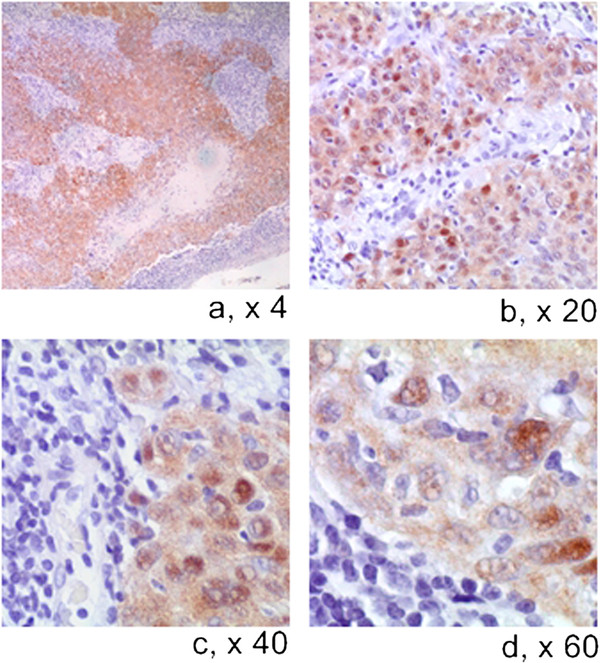
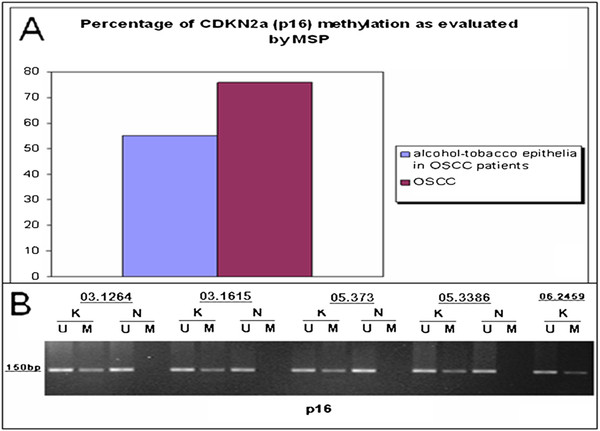
Recent emerging evidences identify Human Papillomavirus (HPV) related Head and Neck squamous cell carcinomas (HN-SCCs) as a separate subgroup among Head and Neck Cancers with different epidemiology, histopathological characteristics, therapeutic response to chemo-radiation treatment and clinical outcome. However, there is not a worldwide consensus on the methods to be used in clinical practice. The endpoint of this study was to demonstrate the reliability of a triple method which combines evaluation of: 1. p16 protein expression by immunohistochemistry (p16-IHC); 2. HPV-DNA genotyping by consensus HPV-DNA PCR methods (Consensus PCR); and 3 viral integration into the host by in situ hybridization method (ISH). This triple method has been applied to HN-SCC originated from oral cavity (OSCC) and oropharynx (OPSCC), the two anatomical sites in which high risk (HR) HPVs have been clearly implicated as etiologic factors. Methylation-Specific PCR (MSP) was performed to study inactivation of p16-CDKN2a locus by epigenetic events. Reliability of multiple methods was measured by Kappa statistics.
All the HN-SCCs confirmed HPV positive by PCR and/or ISH were also p16 positive by IHC, with the latter showing a very high level of sensitivity as single test (100% in both OSCC and OPSCC) but lower specificity level (74% in OSCC and 93% in OPSCC).Concordance analysis between ISH and Consensus PCR showed a faint agreement in OPSCC (κ = 0.38) and a moderate agreement in OSCC (κ = 0.44). Furthermore, the addition of double positive score (ISHpositive and Consensus PCR positive) increased significantly the specificity of HR-HPV detection on formalin-fixed paraffin embedded (FFPE) samples (100% in OSCC and 78.5% in OPSCC), but reduced the sensitivity (33% in OSCC and 60% in OPSCC). The significant reduction of sensitivity by the double method was compensated by a very high sensitivity of p16-IHC detection in the triple approach.
Although HR-HPVs detection is of utmost importance in clinical settings for the Head and Neck Cancer patients, there is no consensus on which to consider the 'golden standard' among the numerous detection methods available either as single test or combinations. Until recently, quantitative E6 RNA PCR has been considered the 'golden standard' since it was demonstrated to have very high accuracy level and very high statistical significance associated with prognostic parameters. In contrast, quantitative E6 DNA PCR has proven to have very high level of accuracy but lesser prognostic association with clinical outcome than the HPV E6 oncoprotein RNA PCR. However, although it is theoretically possible to perform quantitative PCR detection methods also on FFPE samples, they reach the maximum of accuracy on fresh frozen tissue. Furthermore, worldwide diagnostic laboratories have not all the same ability to analyze simultaneously both FFPE and fresh tissues with these quantitative molecular detection methods. Therefore, in the current clinical practice a p16-IHC test is considered as sufficient for HPV diagnostic in accordance with the recently published Head and Neck Cancer international guidelines. Although p16-IHC may serve as a good prognostic indicator, our study clearly demonstrated that it is not satisfactory when used exclusively as the only HPV detecting method. Adding ISH, although known as less sensitive than PCR-based detection methods, has the advantage to preserve the morphological context of HPV-DNA signals in FFPE samples and, thus increase the overall specificity of p16/Consensus PCR combination tests.
最近出现的证据将 HPV 相关头颈部鳞状细胞癌(HN-SCC)确定为头颈部癌症的一个单独亚组,具有不同的流行病学、组织病理学特征、对化疗和放疗治疗的反应以及临床结果。然而,在临床实践中使用的方法尚未达成全球共识。本研究的终点是证明一种三重方法的可靠性,该方法结合了以下三种方法的评估:1. 通过免疫组织化学(p16-IHC)评估 p16 蛋白表达;2. 通过共识 HPV-DNA PCR 方法(Consensus PCR)进行 HPV-DNA 基因分型;3. 通过原位杂交方法(ISH)评估病毒整合到宿主中。该三重方法已应用于来源于口腔(OSCC)和口咽(OPSCC)的 HN-SCC,这两个解剖部位明确涉及高危(HR)HPV 作为病因因素。甲基化特异性 PCR(MSP)用于研究表观遗传事件引起的 p16-CDKN2a 基因座失活。通过 Kappa 统计测量多种方法的可靠性。
所有通过 PCR 和/或 ISH 证实为 HPV 阳性的 HN-SCC 也通过 IHC 显示为 p16 阳性,后者作为单一检测具有非常高的敏感性(在 OSCC 和 OPSCC 中均为 100%),但特异性水平较低(在 OSCC 中为 74%,在 OPSCC 中为 93%)。ISH 和 Consensus PCR 之间的一致性分析显示在 OPSCC 中存在微弱的一致性(κ=0.38),在 OSCC 中存在中度的一致性(κ=0.44)。此外,双阳性评分(ISH 阳性和 Consensus PCR 阳性)的增加显著提高了 HR-HPV 在福尔马林固定石蜡包埋(FFPE)样本中的检测特异性(在 OSCC 中为 100%,在 OPSCC 中为 78.5%),但降低了敏感性(在 OSCC 中为 33%,在 OPSCC 中为 60%)。双方法显著降低的敏感性被三重方法中 p16-IHC 检测的高敏感性所补偿。
尽管 HR-HPV 检测对头颈部癌症患者的临床治疗非常重要,但在众多检测方法中,无论是作为单一检测还是组合检测,都没有一种方法被认为是“金标准”。直到最近,定量 E6 RNA PCR 一直被认为是“金标准”,因为它被证明具有非常高的准确性水平和与预后参数相关的非常高的统计学意义。相比之下,定量 E6 DNA PCR 已被证明具有非常高的准确性水平,但与 HPV E6 致癌蛋白 RNA PCR 相比,与临床结果的预后相关性较低。然而,尽管从理论上讲可以对 FFPE 样本进行定量 PCR 检测方法,但它们在新鲜冷冻组织上达到最高的准确性。此外,全球诊断实验室并非都有能力同时分析这些定量分子检测方法的 FFPE 和新鲜组织。因此,在当前的临床实践中,p16-IHC 检测被认为足以满足 HPV 诊断,符合最近发布的头颈部癌症国际指南。尽管 p16-IHC 可作为良好的预后指标,但我们的研究清楚地表明,当单独用作唯一的 HPV 检测方法时,它并不令人满意。添加 ISH 虽然不如基于 PCR 的检测方法敏感,但具有在 FFPE 样本中保留 HPV-DNA 信号形态学背景的优势,并因此提高了 p16/Consensus PCR 联合检测的整体特异性。