Division of Endocrine Surgery, Department of Surgery, University of Hong Kong, Pokfulam, Hong Kong SAR, China.
World J Surg. 2012 Jun;36(6):1300-6. doi: 10.1007/s00268-012-1561-9.
Post-thyroidectomy hypocalcemia is a major contributing factor in delayed hospital discharge and dissuading surgeons from ambulatory thyroidectomy. We prospectively evaluated the accuracy and reliability of quick parathyroid hormone level measurement at skin closure (PTH-SC) in predicting clinically relevant hypocalcemia (i.e., patients requiring calcium ± calcitriol supplements on hospital discharge).
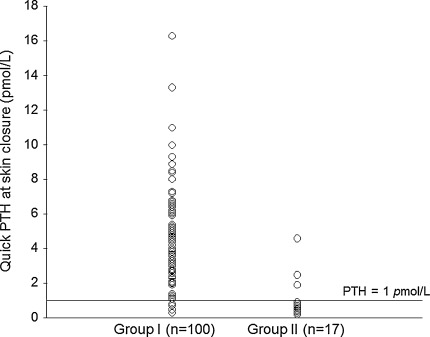
Of the 117 patients who underwent a total or completion total thyroidectomy and PTH-SC, 17 (14.5 %) had hypocalcemic symptoms or adjusted calcium <1.90 mmol/L requiring calcium and/or calcitriol supplements on discharge. Serum calcium was checked regularly in the perioperative period until stabilization and an additional quick PTH was checked on the following morning (PTH-D1). Univariate and multivariate analyses were performed to evaluate potential preoperative clinicopathologic factors and postoperative day 0 biochemical indicators. Youden's index and the area under the ROC curve (AUC) were used to determine the best cutoff value and predictability of significant variables or criteria, respectively.
In the multivariate analysis, low preoperative adjusted calcium (p = 0.041) and low PTH-SC (p = 0.001) were the two independent variables associated with hypocalcemia. PTH-SC (≤1 or >1 pmol/L) had a higher specificity (95.0 %) and AUC (0.887) than serial calcium monitoring or PTH-D1 alone. Although 3/98 of patients with PTH-SC >1 pmol/L required calcium supplements on discharge, they required only the minimum amount to maintain normocalcemia.
PTH-SC is an accurate and reliable means of predicting clinically relevant hypocalcemia. It would be reasonable to discharge those with PTH-SC >1 pmol/L on the same operative day as the risk of life-threatening hypocalcemia would seem unlikely.
甲状腺切除术后低钙血症是导致住院时间延长的主要因素之一,也是阻碍外科医生开展门诊甲状腺切除术的原因之一。我们前瞻性评估了在皮肤缝合时快速甲状旁腺激素水平测量(PTH-SC)预测临床上相关低钙血症(即需要在出院时补充钙和/或骨化三醇的患者)的准确性和可靠性。
在 117 例接受甲状腺全切术或甲状腺全切除术及 PTH-SC 的患者中,有 17 例(14.5%)出现低钙血症症状或调整钙 <1.90mmol/L,需要在出院时补充钙和/或骨化三醇。在围手术期定期检查血清钙,直到稳定,次日(PTH-D1)再检查一次快速甲状旁腺激素。采用单因素和多因素分析评估潜在的术前临床病理因素和术后第 0 天生化指标。采用 Youden 指数和 ROC 曲线下面积(AUC)确定有意义的变量或标准的最佳截断值和预测能力。
在多因素分析中,术前调整钙水平低(p=0.041)和 PTH-SC 低(p=0.001)是与低钙血症相关的两个独立变量。PTH-SC(≤1 或>1pmol/L)的特异性(95.0%)和 AUC(0.887)均高于单独进行血清钙监测或 PTH-D1。尽管有 3/98 例 PTH-SC>1pmol/L 的患者在出院时需要补充钙,但只需补充最低剂量即可维持正常血钙水平。
PTH-SC 是预测临床上相关低钙血症的一种准确可靠的方法。对于 PTH-SC>1pmol/L 的患者,在同一天出院是合理的,因为发生危及生命的低钙血症的风险似乎不大。