Division of Endocrinology, Diabetes, Metabolism, and Nutrition, Mayo Clinic, Rochester, Minnesota, USA.
Diabetes. 2012 May;61(5):1082-9. doi: 10.2337/db11-1732. Epub 2012 Mar 28.
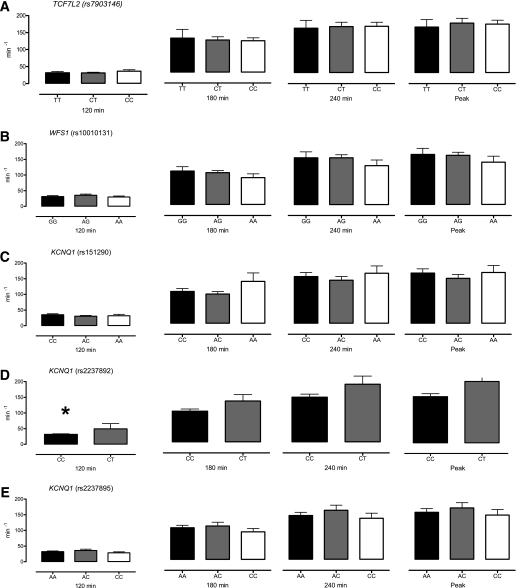
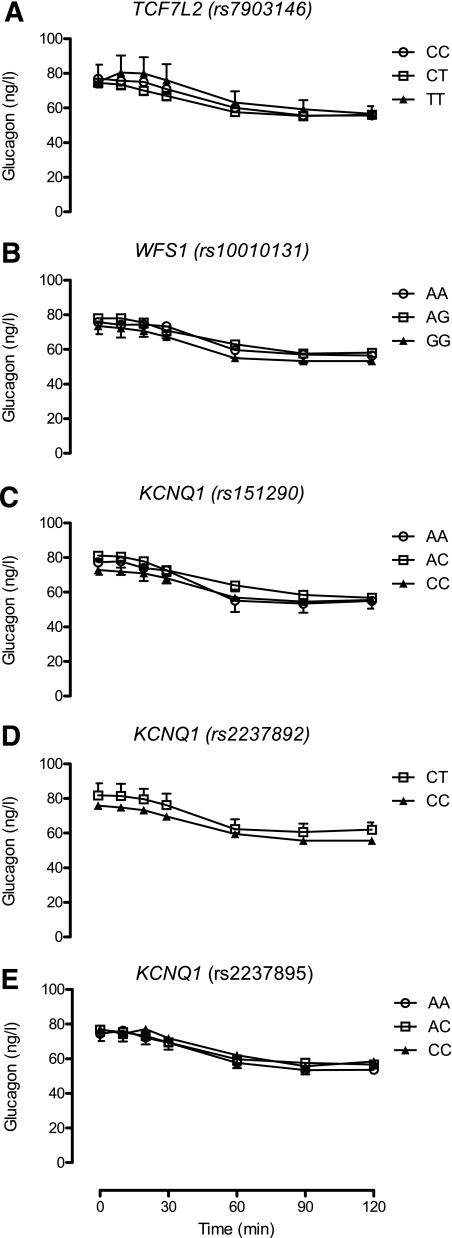
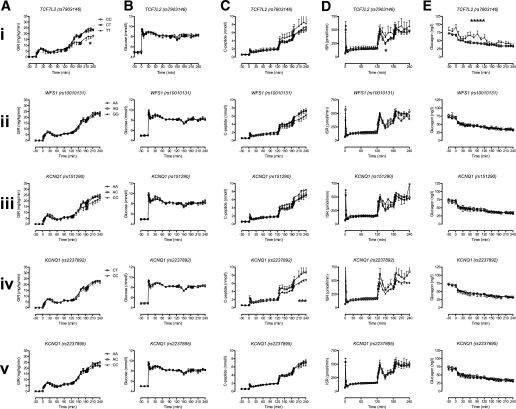
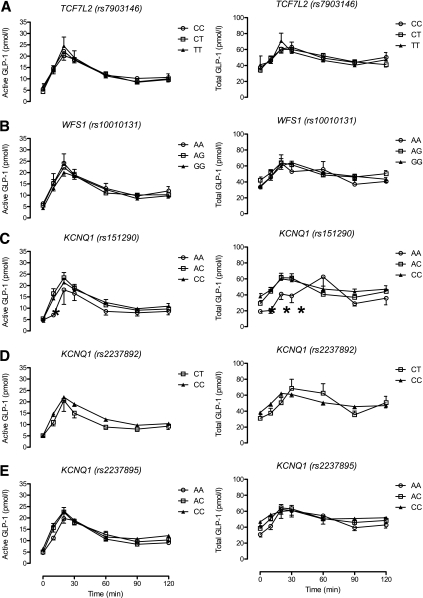
The mechanisms by which common genetic variation predisposes to type 2 diabetes remain unclear. The disease-associated variants in TCF7L2 (rs7903146) and WFS1 (rs10010131) have been shown to affect response to exogenous glucagon-like peptide 1 (GLP-1), while variants in KCNQ1 (rs151290, rs2237892, and rs2237895) alter endogenous GLP-1 secretion. We set out to validate these observations using a model of GLP-1-induced insulin secretion. We studied healthy individuals using a hyperglycemic clamp and GLP-1 infusion. In addition, we measured active and total GLP-1 in response to an oral challenge in nondiabetic subjects. After genotyping the relevant single nucleotide polymorphisms, generalized linear regression models and repeated-measures ANCOVA models incorporating potential confounders, such as age and BMI, were used to assess the associations, if any, of response with genotype. These variants did not alter GLP-1 concentrations in response to oral intake. No effects on β-cell responsiveness to hyperglycemia and GLP-1 infusion were apparent. Diabetes-associated variation (T allele at rs7903146) in TCF7L2 may impair the ability of hyperglycemia to suppress glucagon (45 ± 2 vs. 47 ± 2 vs. 60 ± 5 ng/L for CC, CT, and TT, respectively, P = 0.02). In nondiabetic subjects, diabetes-associated genetic variation does not alter GLP-1 concentrations after an oral challenge or its effect on insulin secretion.
常见遗传变异导致 2 型糖尿病的机制仍不清楚。TCF7L2(rs7903146)和 WFS1(rs10010131)的疾病相关变异被证明会影响对外源性胰高血糖素样肽 1(GLP-1)的反应,而 KCNQ1(rs151290、rs2237892 和 rs2237895)的变异会改变内源性 GLP-1 的分泌。我们使用 GLP-1 诱导的胰岛素分泌模型来验证这些观察结果。我们使用高血糖钳夹和 GLP-1 输注研究了健康个体。此外,我们还在非糖尿病患者中测量了口服挑战时活性和总 GLP-1 的反应。在对相关单核苷酸多态性进行基因分型后,使用广义线性回归模型和包含年龄和 BMI 等潜在混杂因素的重复测量 ANCOVA 模型来评估基因型与反应之间的关联(如果有的话)。这些变体不会改变口服摄入后 GLP-1 的浓度。对高血糖和 GLP-1 输注引起的β细胞反应没有明显影响。TCF7L2 中的糖尿病相关变异(rs7903146 的 T 等位基因)可能会损害高血糖抑制胰高血糖素的能力(CC、CT 和 TT 分别为 45±2、47±2 和 60±5ng/L,P=0.02)。在非糖尿病患者中,糖尿病相关遗传变异不会改变口服挑战后的 GLP-1 浓度及其对胰岛素分泌的影响。